1. Aboriginal sexual health: The Australian : Was the syphilis epidemic preventable ? NACCHO responds
2.Royal Flying Doctors Service extra 4-year funding $84 million Mental Health and Dental Services
3.Nurses PAQ continues political membership campaign spreading false and misleading information about our cultural safety
4.AMSANT has called for re-doubled efforts to implement the recommendations of the Royal Commission into the care and protection of children in partnership with NT Aboriginal leaders
5.Dialysis facilities worth $17 million are sitting padlocked, empty and unused in WA’s north
6.ALRC Report into Incarceration of Aboriginal and Torres Strait Islander People.
7. Minister Ken Wyatt : Listening to Indigenous Needs: Healthy Ears Program Extended with $29.4 commitment
8.Tangentyere Alice Springs Women’s Family Safety Group visits Canberra
9.Minister Ken Wyatt launches our NACCHO RACGP National Guide to a preventative health assessment for Aboriginal and Torres Strait Islander people
10. Your guide to a healthy Easter : #Eggs-actly
1.Aboriginal sexual health: The Australian : Was the syphilis epidemic preventable ? NACCHO responds
“These (STIs) are preventable diseases and we need increased testing, treatment plans and a culturally appropriate health education campaign that focuses resources on promoting safe-sex messages delivered to at-risk communities by our trained Aboriginal workforce,”
Pat Turner, chief executive of peak body the National Aboriginal Community Controlled Health Organisation, is adamant about this.
4. AMSANT has called for re-doubled efforts to implement the recommendations of the Royal Commission into the care and protection of children in partnership with NT Aboriginal leaders
7. Minister Ken Wyatt : Listening to Indigenous Needs: Healthy Ears Program Extended with $29.4 commitment
The Australian Government has committed $29.4 million to extend the Healthy Ears – Better Hearing, Better Listening Program, to help ensure tens of thousands more Indigenous children and young adults grow up with good hearing and the opportunities it brings.
8.Tangentyere Alice Springs Women’s Family Safety Group visits Canberra
This week the Tangentyere Women’s Family Safety Group from Alice Springs were in Canberra. They shared with politicians, their own solutions for their own communities, and they are making an enormous difference.
Big thanks to all the Tangentyere women who made it to Canberra.
And finally hope you had a Happy Easter all you mob ! After you have enjoyed your chocolate #Easter eggs and hot cross buns , this is how much exercise you will require to work of those Easter treats .
For medical and nutrition advice please check with your ACCHO Doctor , Health Promotion / Lifestyle teams or one of our ACCHO nutritionists
There is no reason it should have happened, especially not in a first-world country like Australia, but it has: indigenous communities in the country’s north are in the grip of wholly treatable sexually transmitted diseases.
In the case of syphilis, it is an epidemic — West Australian Labor senator Patrick Dodson described it as such, in a fury, when health department bureaucrats mumbled during Senate estimates about having held a few “meetings” on the matter.
There have been about 2000 syphilis notifications — with at least 13 congenital cases, six of them fatal — since the outbreak began in northern Queensland in 2011, before spreading to the Northern Territory, Western Australia and, finally, South Australia.
What’s worse, it could have been stopped. James Ward, of the South Australian Health and Medical Research Institute, wrote in mid-2011 that there had been a “downward trend” over several years and it was likely at that point that the “elimination of syphilis is achievable within indigenous remote communities”.
But governments were slow to react, and Ward is now assisting in the design of an $8.8 million emergency “surge” treatment approach on the cusp of being rolled out in Cairns and Darwin, with sites in the two remaining affected states yet to be identified.
It will be an aggressive strategy — under previous guidelines, you had to have been identified during a health check as an active carrier of syphilis to be treated. Now, anyone who registers antibodies for the pathogen during a blood prick test, whether actively carrying syphilis or not, will receive an immediate penicillin injection in an attempt to halt the infection’s geographical spread.
This is key: the high mobility of indigenous people in northern and central Australia means pathogens cross jurisdictions with impunity. Australian Medical Association president Michael Gannon calls syphilis a “clever bacterium that will never go away”, warning that “bugs don’t respect state borders”.
Olga Havnen, one of the Northern Territory’s most respected public health experts, points out that many people “will have connections and relations from the Torres Strait through to the Kimberley and on to Broome — and it’s only a matter of seven or eight kilometres between PNG and the northernmost islands there in the Torres Strait”.
“This is probably something that’s not really understood by the broader Australian community,” Havnen says. “I suspect once you get a major outbreak of something like encephalitis or Dengue fever, any of those mosquito-borne diseases, and that starts to encroach onto the mainland, then people will start to get a bit worried.”
Olga Havnen, CEO of the Danila Dilba Health Service, says transmission is complex issue in Australia’s indigenous communities.
But it is not just syphilis — indeed, not even just STIs — that have infectious disease authorities concerned and the network of Aboriginal Community Controlled Health Organisations stretched.
Chlamydia, the nation’s most frequently diagnosed STI in 2016 based on figures from the Kirby Institute at the University of NSW, is three times more likely to be contracted by an indigenous Australian than a non-indigenous one.
The rate was highest in the NT, at 1689.1 notifications per 100,000 indigenous people, compared with 607.9 per 100,000 non-indigenous Territorians. If you’re indigenous, you’re seven times more likely to contract gonorrhoea, spiking to 15 times more likely if only women are considered. Syphilis, five times more likely.
As the syphilis response gets under way, health services such as the one Havnen leads, the Darwin-based Danila Dilba, will be given extra resources to tackle it. “With proper resourcing, if you want to be doing outreach with those people who might be visitors to town living in the long grass, then we’re probably best placed to be able to do that,” she says.
But the extra focus comes with a warning. A spate of alleged sexual assaults on Aboriginal children, beginning with a two-year-old in Tennant Creek last month and followed by three more alleged attacks, has raised speculation of a link between high STI rates and evidence of child sexual assault.
After the first case, former NT children’s commissioner Howard Bath told this newspaper that STI rates were “a better indicator of background levels of abuse than reporting because so many of those cases don’t get reported to anyone, whereas kids with serious infections do tend to go to a doctor”. Others, including Alice Springs town councillor Jacinta Price and Aboriginal businessman Warren Mundine, raised the spectre of the need for removing more at-risk indigenous children from dangerous environments.
Children play AFL in Yeundumu. Picture: Jason Edwards
However, Sarah Giles, Danila Dilba’s clinical director and a medical practitioner of 20 years’ standing in northern Australia, warns this kind of response only exacerbates the problem. She is one of a range of public health authorities who, like Havnen, say connecting high STI figures to the very real scourge of child sex abuse simply makes no sense. They do not carry correlated data sets, the experts say.
“One of the things that’s really unhelpful about trying to manage STIs at a population level is to link it with child abuse and mandatory reporting, and for people to be fearful of STIs,” Giles says. “The problem is that when they’re conflated and when communities feel that they can’t get help because things might be misinterpreted or things might be reported, they’re less likely to present with symptoms. The majority of STIs are in adults and they’re sexually transmitted.”
Havnen says there is evidence of STIs being transmitted non-sexually, including to children, such as through poor hand hygiene, although Giles says that is “reasonably rare”. And while NT data shows five children under 12 contracted either chlamydia or gonorrhoea in 2016 (none had syphilis), and there were another five under 12 last year, Havnen points to the fact that over the past decade there has been no increasing trend in under 12s being affected. Where there has been a rise in the NT is in people aged between 13 and 19, with annual gonorrhoea notifications increasing from 64 cases in the 14-15-year-old female cohort in 2006 to 94 notifications in 2016.
In the 16-17-year-old female cohort the same figures were 96 and 141 and in the 12-13-year-old group it rose from 20 in 2006 to 33 in 2016. Overall, for both boys and girls under 16, annual gonorrhoea notifications rose from 109 in 2006 to 186 in 2016, according to figures provided to the royal commission into child detention by NT Health. Havnen describes the rise as “concerning but not, on its own, evidence of increasing levels of sexual abuse”.
Ward is more direct. Not all STIs are the result of sexual abuse, he warns, and not all sexual abuse results in an STI. If you’re a health professional trying to deal with an epidemiological wildfire, the distinction matters — the data and its correct interpretations can literally be a matter of life and death.
Indeed, in its own written caveats to the material it provided to the royal commission, the department warns that sexual health data is “very much subject to variations in testing” and warns against making “misleading assumptions about trends”. Ward says: “Most STIs notified in remote indigenous communities are assumed to be the result of sex between consenting adults — that is, 16 to 30-year-olds. Of the under 16s, the majority are 14 and 15-year-olds.” He says a historically high background prevalence of STIs in remote indigenous communities — along with a range of other infectious diseases long eradicated elsewhere — is to blame for their ongoing presence. Poor education, health services and hygiene contribute, and where drug and alcohol problems exist, sexually risky behaviour is more likely too. The lingering impact of colonisation and arrival of diseases then still common in broader society cannot be underestimated.
But Ward claims that an apparently high territory police figure of about 700 cases of “suspected child sexual offences” in the NT over the past five years may be misleading. He says a large number of these are likely to be the result of mandatory reporting, where someone under 16 is known to have a partner with an age gap of more than two years, or someone under 14 is known to be engaging in sexual activity. Ward points out that 15 is the nationwide median sexual debut age, an age he suggests is dropping. At any rate, he argues, child sex abuse is unlikely to be the main reason for that high rate of mandatory reporting in the NT.
Areyonga is a small Aboriginal community a few hours drive from Alice Springs.
Data matters, and so does how it is used. Chipping away at the perception of child sexual abuse in indigenous communities are the latest figures from the Australian Institute of Health and Welfare showing the rate of removals for that crime is actually higher in non-indigenous Australia.
According to a report this month from the AIHW, removals based on substantiated sex abuse cases in 2016-17 were starkly different for each cohort: 8.3 per cent for indigenous children, from a total of 13,749 removals, and 13.4 per cent for non-indigenous children, from 34,915 removals.
Havnen concedes there is a need for better reporting of child abuse and has called for a confidential helpline that would be free of charge and staffed around the clock by health professionals.
It’s based on a model already in use in Europe that she says deals with millions of calls a year — but it would require a comprehensive education and publicity campaign if it were to gain traction in remote Australia. And that means starting with the adults.
“If you’re going to do sex education in schools and you start to move into the area about sexual abuse and violence and so on, it’s really important that adults are educated first about what to do with that information,” she says. “Because too often if you just educate kids, and they come home and make a disclosure, they end up being told they’re liars.”
These challenges exist against the backdrop of a community already beset by a range of infectious diseases barely present elsewhere in the country, including the STIs that should be so easily treatable. It is, as Havnen is the first to admit, a complex matter.
Cheryl Jones, president of the Australasian Society for Infectious Diseases, says the answer is better primary treatment solutions and education, rather than trying to solve the problem after it has occurred. “For any of these public health infectious disease problems in remote and rural areas, we need to support basic infrastructure at the point of care and work alongside communities to come up with solutions,” she says.
Sisters play in the mud after a rare rain at Hoppy’s ‘town camp’ on the outskirts of Alice Springs.
Pat Turner, chief executive of peak body the National Aboriginal Community Controlled Health Organisation, is adamant about this. “These (STIs) are preventable diseases and we need increased testing, treatment plans and a culturally appropriate health education campaign that focuses resources on promoting safe-sex messages delivered to at-risk communities by our trained Aboriginal workforce,” Turner says.
The Australian Medical Association has called for the formation of a national Centre for Disease Control, focusing on global surveillance and most likely based in the north, as being “urgently needed to provide national leadership and to co-ordinate rapid and effective public health responses to manage communicable diseases and outbreaks”.
“The current approach to disease threats, and control of infectious diseases, relies on disjointed state and commonwealth formal structures, informal networks, collaborations, and the goodwill of public health and infectious disease physicians,” the association warned in a submission to the Turnbull government last year.
However, the federal health department has rebuffed the CDC argument, telling the association that “our current arrangements are effective” and warning the suggestion could introduce “considerable overlap and duplication with existing functions”.
“I think it (the CDC) might have some merit, if it helps to advocate with government about what needs to happen,” Havnen says, “but if these things are going to be targeted at Aboriginal bodies, it needs to be a genuine partnership. It’s got to be informed by the realities on the ground and what we know. That information has to be fed up into the planning process.”
“All of our 6000 staff in 145 member services in 305 health settings across Australia will have access to this new and update edition of the National Guide. It’s a comprehensive edition for our clinicians and support staff that updates them all with current medical practice.
“NACCHO is committed to quality healthcare for Aboriginal and Torres Strait Islander patients, and will work with all levels of government to ensure accessibility for all.”
NACCHO Chair John Singer said the updated National Guide would help governments improve health policy and lead initiatives that support Aboriginal and Torres Strait Islander people.
A/Prof Peter O’Mara, NACCHO Chair John Singer Minister Ken Wyatt & RACGP President Dr Bastian Seidel launch the National guide at Parliament house this morning
“Prevention is always better than cure. Already one of the most widely used clinical guidelines in Australia, this new edition includes critical information on lung cancer, Foetal Alcohol Spectrum Disorder and preventing child and family abuse and violence.
The National Guide maximises the opportunities at every clinic visit to prevent disease and to find it early.It will help increase vigilance over previously undiagnosed conditions, by promoting early intervention and by supporting broader social change to help individuals and families improve their wellbeing.”
Minister Ken Wyatt highlights what is new to the 3rd Edition of the National Guide-including FASD, lung cancer, young people lifecycle, family abuse & violence and supporting families to optimise child safety & wellbeing : Pic Lisa WhopSEE Full Press Release Part 2 Below
The Royal Australian College of General Practitioners (RACGP) and the National Aboriginal Community Controlled Health Organisation (NACCHO) have joined forces to produce a guide that aims to improve the level of healthcare currently being delivered to Aboriginal and Torres Strait Islander patients and close the gap.
Chair of RACGP Aboriginal and Torres Strait Islander Health Associate Professor Peter O’Mara said the third edition of the National guide to a preventive health assessment for Aboriginal and Torres Strait Islander people (the National Guide) is an important resource for all health professionals to deliver best practice healthcare to Aboriginal and Torres Strait Islander patients.
“The National Guide will support all healthcare providers, not just GPs, across Australia to improve prevention and early detection of disease and illness,” A/Prof O’Mara said.
“The prevention and early detection of disease and illness can improve people’s lives and increase their lifespans.
“The National Guide will support healthcare providers to feel more confident that they are looking for health issues in the right way.”
RACGP President Dr Bastian Seidel said the RACGP is committed to tackling the health disparities between Indigenous and non-Indigenous Australians.
“The National Guide plays a vital role in closing the gap in Aboriginal and Torres Strait Islander health disparity,” Dr Seidel said.
“Aboriginal and Torres Strait Islander people should have equal access to quality healthcare across Australia and the National guide is an essential part of ensuring these services are provided.
“GPs and other healthcare providers who implement the recommendations within the National Guide will play an integral role in reducing health disparity between Indigenous and non-Indigenous Australians, and ensuring culturally responsive and appropriate healthcare is always available.”
The updated third edition of the National Guide can be found on the RACGP website and the NACCHO website.
Free to download on the RACGP website and the NACCHO website:
Part 2 Prevention and Early Diagnosis Focus for a Healthier Future
The critical role of preventive care and tackling the precursors of chronic disease is being boosted in the latest guide for health professionals working to close the gap in health equality for Indigenous Australians
The critical role of preventive care and tackling the precursors of chronic disease is being boosted in the latest guide for health professionals working to close the gap in health equality for Indigenous Australians.
Minister for Indigenous Health, Ken Wyatt AM, today launched the updated third edition of the National guide to a preventive health assessment for Aboriginal and Torres Strait Islander people.
“Prevention is always better than cure,” said Minister Wyatt. “Already one of the most widely used clinical guidelines in Australia, this new edition includes critical information on lung cancer, Foetal Alcohol Spectrum Disorder and preventing child and family abuse and violence.
“The National Guide maximises the opportunities at every clinic visit to prevent disease and to find it early.
“It will help increase vigilance over previously undiagnosed conditions, by promoting early intervention and by supporting broader social change to help individuals and families improve their wellbeing.”
The guide, which was first published in 2005, is a joint project between the National Aboriginal Community Controlled Health Organisation (NACCHO) and the Royal Australian College of General Practitioners RACGP).
“To give you some idea of the high regard in which it is held, the last edition was downloaded 645,000 times since its release in 2012,” said Minister Wyatt.
“The latest edition highlights the importance of individual, patient-centred care and has been developed to reflect local and regional needs.
“Integrating resources like the national guide across the whole health system plays a pivotal role in helping us meet our Closing the Gap targets.
“The Turnbull Government is committed to accelerating positive change and is investing in targeted activities that have delivered significant reductions in the burden of disease.
“Rates of heart disease, smoking and binge drinking are down. We are on track to achieve the child mortality target for 2018 and deaths associated with kidney and respiratory diseases have also reduced.”
The National Guide is funded under the Indigenous Australian’s Health Programme as part of a record $3.6 billion investment across four financial years.
The RACGP received $429,000 to review, update, publish and distribute the third edition, in hard copy and electronic formats.
” The sexual abuse of any Aboriginal or non-Aboriginal children has got to stop.
It is not acceptable and in no way can our communities, the Australian community at large or Governments at all levels condone this continuing.
I welcome a thorough investigation by the Northern Territory Child Abuse Taskforce and Children’s Commissioner into this grave allegation.”
The National Aboriginal Community Controlled Health Organisation(NACCHO ) Chair John Singer said he is deeply concerned that some of our children are being sexually interfered with.
“According to media reports last this week, a four-year-old boy from the community of Ali Curung in the Northern Territory has been taken to Alice Springs for medical care after he was allegedly sexually assaulted on the weekend and police are investigating.”
See The Guardian article Part 2 Below
” High levels of disadvantage, alongside “vulnerable and very impoverished” communities, was putting children at risk.
What’s really tragic is that we’ve known about them [problems] for well over a decade and more, and there’s been very little sustained, concerted effort to deal with them,
What’s absolutely needed are more of the early intervention and prevention programs, better parenting programs, and a better level of education and awareness about child.”
Chief executive of the Danila Dilba Aboriginal Medical Service, Olga Havnen, is unsurprised by the most recent incident : Interview ABC
” The community was devastated, but not surprised by the latest allegations, and there had been a feeling of “absolute hopelessness” as community leaders beared witness to social dysfunction, alcohol abuse and child protection problems.
They are issues which are attribute to overcrowded public housing.
Resourcing across all sectors and services is what’s needed to support vulnerable families,
I think it’s just been a build-up of years and years of neglect and limited resources.”
At least 40 extra houses were needed in the area to reduce overcrowding, and reduce the risk for children.
It just allows for an explosion, if you like, to further dysfunction of Aboriginal families.
[It] just leads to total hopelessness… creating such incidents as what’s happening now where our children are being harmed.”
Barb Shaw, the chief executive of the Anyinginyi Health Aboriginal Corporation, which takes in Ali Curung.
#WeHaveTheSolutions :Government must take off the blinkers over these issues, show leadership and take the actions outlined.
1.Immediate Government actionto assist families to keep their children safe. We know these are complex issues requiring urgent responses but the abuse still continues.
2.We need a comprehensive approachto child and community safety with a focus on prevention and community education.
3. Establishing a Confidential Child Help Linewithin Aboriginal Community Controlled Health Services by regions which is a no-brainer for any government to fund and implement in this budget cycle.
In getting better rates of disclosure, we can respond to both victims and offenders. This is particularly important when young people are perpetrators so that they can be held to account for their behaviour and receive appropriate rehabilitation and behavioural change programs.
4.Extra resources should also be made immediately available for wrap around Families and Children Support services to work with traumatised children and their families. This requires a multi-disciplinary professional team to provide full assessment and treatment programs in our local communities. A health-led therapeutic model will deliver much better outcomes for our people.
Often as the academic evidence now suggests, perpetrators have themselves often been abused and they too require treatment not punitive punishment regimes or they will not be rehabilitated and will re-offend.
5.National plan to redress the Social Determinantsof Health in Aboriginal communities throughout Australia.[1]
6.Liquor licenses :The NT Government needs to take a good hard look at the total number of liquor licenses granted and curtail them to stop the flow of alcohol. People must come before profits. The grog is killing our people and our children are exposed to the results of that every day.
Those dry communities are to be commended for their efforts to control alcohol consumption, but the sheer number of liquor outlets at Roadhouses on the Highway and in the closest towns undermines their efforts to live safe and peacefully in their local community. Government must take off the blinkers over these issues, show leadership and take the actions outlined,” said Mr Singer.
Part 2 Boy, 16, charged with rape of four-year-old boy in remote Northern Territory community
Noting NACCHO press release was published in online article
A 16-year-old boy has been charged over the alleged rape of a four-year-old boy in a remote Northern Territory community.It is at least the second such incident in the Barkly region, after a two-year-old girl was sexually assaulted in Tennant Creek last month.
The 16-year-old is scheduled to appear in the Alice Springs youth court on Tuesday, to face one charge of sexual intercourse without consent.
The NT police child abuse taskforce was investigating the alleged attack, which reportedly occurred on Sunday, and said it was not seeking anyone else in relation to the matter.
The territory families minister, Dale Wakefield, said a full team of staff was on the ground as part of the child abuse taskforce.
“They are working alongside police and engaging with the family and the community,” she said.
“We have also spoken to the children’s commissioner and will keep her informed of any developments.
“It is heartbreaking for any child anywhere to be harmed. Every child deserves a childhood where they are safe and given pathways to reach their full potential.”
A 24-year-old charged with sexually assaulting a two-year-old in Tennant Creek is scheduled to appear in court in April.
That alleged incident prompted emergency measures by NT authorities, including the immediate deployment of extra Territory Families department staff and the implementation of strict alcohol restrictions on Tennant Creek.
The community where the latest alleged assault happened is one of about 100 in the NT with restrictions or bans on drinking alcohol.
Steve Edgington, the mayor of Tennant Creek, said there had been “immediate learnings” after the alleged assault in his town.
Edgington said there was a clear need to decentralise government resources and divert them to identified hotspots of disadvantage.
“What needs to be done is a full audit of where these particular incidents are happening,” he said.
“I’m sure they’re happening elsewhere. We need to allocate resources to where these incidents are, tackling issues from the ground up. It’s just critical – children need to be safe in our communities.”
Edgington said most resources in the Barkly region were based in Tennant Creek and there were a number of small remote communities nearby where governments could look at what resources were allocated for child protection and welfare, housing, and other areas.
On Monday the NT chief minister, Michael Gunner, said extra Territory Families staff had been deployed to the community and the incident would also be referred to the children’s commissioner.
“This is an extremely disturbing incident,” he told the ABC. “Every child, no matter where they live, deserves to be in a safe environment.”
1. 2018 NACCHO Annual Members’ Conference and AGM SAVE A DATE
Follow our conference using HASH TAG #NACCHOagm2018
This is Brisbane Oct 30—Nov 2
The NACCHO Members’ Conference and AGM provides a forum for the Aboriginal community controlled health services workforce, bureaucrats, educators, suppliers and consumers to:
Present on innovative local economic development solutions to issues that can be applied to address similar issues nationally and across disciplines
Have input and influence from the ‘grassroots’ into national and state health policy and service delivery
Demonstrate leadership in workforce and service delivery innovation
Promote continuing education and professional development activities essential to the Aboriginal community controlled health services in urban, rural and remote Australia
Promote Aboriginal health research by professionals who practice in these areas and the presentation of research findings
Develop supportive networks
Promote good health and well-being through the delivery of health services to and by Indigenous and non-Indigenous people throughout Australia.
3. NATSIHWA National Professional Development Symposium 2018
We’re excited to release the dates for the 2018 National Professional Development Symposium to be held in Alice Springs on 2nd-4th October. More details are to be released in the coming weeks; a full sponsorship prospectus and registration logistics will be advertised asap via email and newsletter.
This years Symposium will be focussed on upskilling our Aboriginal and/or Torres Strait Islander Health Workers and Health Practitioners through a series of interactive workshops. Registrants will be able to participate in all workshops by rotating in groups over the 2 days. The aim of the symposium is to provide the registrants with new practical skills to take back to communities and open up a platform for Health Workers/Practitioners to network with other Individuals in the workforce from all over Australia.
Building on the foundations of our membership, history and diversity, AIDA is shaping a future where we continue to innovate, lead and stay strong in culture. It’s an exciting time of change and opportunity in Indigenous health.
The AIDA conference supports our members and the health sector by creating an inspiring networking space that engages sector experts, key decision makers, Indigenous medical students and doctors to join in an Indigenous health focused academic and scientific program.
AIDA recognises and respects that the pathway to achieving equitable and culturally-safe healthcare for Indigenous Australians is dynamic and complex. Through unity, leadership and collaboration, we create a future where our vision translates into measureable and significantly improved health outcomes for our communities. Now is the time to put that vision into action.
AIDA Awards
Nominate our members’ outstanding contributions towards improving the health and life outcomes of Aboriginal and Torres Strait Islander Peoples.
We invite you to be part of the CATSINaM Professional Development Conference held in Adelaide, Australia from the 17th to the 19th of September 2018.
The Conference purpose is to share information while working towards an integrated approach to improving the outcomes for Aboriginal and Torres Strait Islander Australians. The Conference also provides an opportunity to highlight the very real difference being made in Aboriginal and Torres Strait Islander health by our Members.
To this end, we are offering a mixed mode experience with plenary speaker sessions, panels, and presentations as well as professional development workshops.
The CATSINaM Gala Dinner and Awards evening, held on the 18th of September, purpose is to honour the contributions of distinguished Members to the field.
7.Study Question: What would it take to address Family Violence in Aboriginal and Torres Strait Islander Communities?
The Australian National University is seeking partnerships with Aboriginal and Torres Strait Islander communities to conduct research to find out what communities need to promote and improve safety for families. We want to partner and work with local organisations and communities to make sure the research benefits the community.
Who are we?
We work at the Australian National University (ANU). The study is led by Aboriginal and Torres Strait Islander researchers. Professor Victoria Hovane (Ngarluma, Malgnin/Kitja, Gooniyandi), along with Associate Professor Raymond Lovett (Wongaibon, Ngiyampaa) and Dr Jill Guthrie (Wiradjuri) from NCEPH, and Professor Matthew Gray of the Centre for Social Research and Methods (CSRM) at ANU will be leading the study.
Study Question: What would it take to address Family Violence in Aboriginal and Torres Strait Islander Communities?
How are we going to gather information to answer the study question?
A Community Researcher (who we would give funds to employ) would capture the data by interviewing 100 community members, running 3 focus groups for Men / Women / Youth (over 16). We would interview approx. 5 community members to hear about the story in your community.
We know Family Violence happens in all communities. We don’t want to find out the prevalence, we want to know what your communities needs to feel safe. We will also be mapping the services in your community, facilities and resources available in a community. All this information will be given back to your community.
What support would we provide your service?
We are able to support your organisation up to $40,000 (including funds for $30 vouchers), this would also help to employ a Community Researcher.
Community participants would be provided with a $30 voucher to complete a survey, another $30 for the focus group, and another $30 for the interview for their time.
What will we give your organisation?
We can give you back all the data that we have captured from your community, (DE identified and confidentialised of course). We can give you the data in any form you like, plus create a Community Report for your community. There might be some questions you would like to ask your community, and we can include them in the survey.
How long would we be involved with your community / organisation?
Approximately 2 months
How safe is the data we collect?
The data is safe. It will be DE identified and Confidentialised. Our final report will reflect what Communities (up to 20) took part in the study, but your data and community will be kept secret. Meaning, no one will know what data came from your community.
Application close April 27
If you think this study would be of benefit to your community, or if you have any questions, please do not hesitate to contact Victoria Hovane, or the teamon 1300 531 600 or email facts.study@anu.edu.au.
Survey – Have your say on the national Key Performance Indicators
Summer May Finlay is currently undertaking a PhD on the impact of the national Key Performance Indicators on the ACCHO sector titled: Defining our own outcomes.
Summer is interested in your views about the Aboriginal Community Controlled Health Organisations (ACCHOs) national Key Performance Indicators (nKPIs) and how these work in your organisation.
To understand what is happening at ACCHOs across the country, she is asking staff who play a role in collecting, reporting or using nKPI data to complete a survey.
The survey will only take about 10 minutes and no person or organisation will be identified in any reporting.
Please feel free to send this email to your staff. The survey will close on the 31st of March.
Attached is the participant information sheet for more information about the research project and the survey. If you have any questions, please don’t hesitate to get in contact with me.
PhD Candidate (Wardliparingga Aboriginal Research Unit, South Australian Health and Medical Research Institute, Adelaide, Centre for Population Health Research, within School of Health Sciences University of South Australia)
Aboriginal and Torres Strait Islander Special Interest Group Co-Convener (Public Health Association of Health)
Co-vice chair Indigenous Working Group (World Federation of Public Health Associations)
” National media outlets ( Including Peta Credlin on SkyNews and News Corp Newspapers see Part 5 below plus Today Tonight SA ) have aired wrongful claims that the codes would force white nurses to ‘apologise to Indigenous clients for being white’.
The codes do not say that – that idea was invented and then pushed on these media programs.
These stories were not based in facts, but seem to have been driven by the partisan politics of a fringe nursing group, and conservative politicians who have been approached to comment on the wrongful claims.
I am sure that some of our nursing and midwifery members and community will be hearing disturbing claims.
Let me be clear, nurses and midwives under the new code do not have to announce their ‘white privilege’ before treating Indigenous clients.
I am really proud of these new codes, and not only because the Congress of Aboriginal and Torres Strait Islander Nurses and Midwives (CATSINaM) contributed to their development, which included extensive consultation across nursing and midwifery and at the time no one opposed the inclusion of cultural safety “
Janine Mohamed CEO CATSINaM see IndigenousX Part 1 below
” It is clear from the 2018 Closing the Gap Report tabled by Prime Minister Turnbull in February 2018 that Aboriginal and/or Torres Strait Islander Peoples still experience poorer health outcomes than non-Indigenous Australians.
It is well understood these inequities are a result of the colonisation process and the many discriminatory policies to which Aboriginal and/or Torres Strait Islander Australians were subjected to, and the ongoing experience of discrimination today.
All healthcare leaders and health professionals have a role to play in closing the gap.
The approach the NMBA has taken for nurses and midwives (the largest workforce in the healthcare system) by setting expectations around culturally safe practice, reflects the current expectations of governments to provide a culturally safe health system.
Combined Press Release Nursing and Midwifery Board of Australia ,The Australian Nursing and Midwifery Federation, the Australian College of Nursing, the Australian College of Midwives and the Congress of Aboriginal and Torres Strait see in full Part 2 Below
” I was stunned to read businessman Graeme Haycroft’s comments regarding nurses and indigenous Australians on the weekend, as part of his criticism of the new NMBA Codes and the term cultural safety which is defined in a glossary connected to the codes.
These codes were the subject of lengthy consultations with the professions of nursing and midwifery and other stakeholders including community representatives.
This review was comprehensive and evidenced-based. Our union and our national body the Australian Nursing Midwifery Federation (ANMF) were active participants in these consultations.
The codes, written by nurses and midwives for nurses and midwives, seek to ensure the individual needs and backgrounds of each patient are taken into account during treatment.”
QNMU Secretary Beth Mohle issued a statement clarifying misleading comments in the media around the NMBA’s new Codes of Conduct for nurses and midwives: See in Full part 3 Below
” And just to reinforce that point, the entire premise for the segment was false.
There is no requirement for nurses to apologise for being white, which would be very awkward for the more the more than 1500 Indigenous nurses across Australia, and the countless others who also aren’t white to begin with. But, even for the nurses who are – THERE IS NO REQUIREMENT FOR THEM TO APOLOGISE FOR BEING WHITE.
So, why on Earth would Today Tonight run such a story?
Why would they base a story off the demonstrably false allegations of this Graeme Haycroft person? “
The truth behind the Nursing Code of Conduct lie ; Indigenous X Article Read in full Part 4
Catch Up: Having to apologise for being white – the controversial new code for nurses treating Indigenous Australians. #TTAdelaidepic.twitter.com/yViiqkw67F
” I’VE seen a lot of crazy political correctness in my time but the new Nurses’ Code of Conduct is right up there with the worst of it.
If you thought nursing was about quality health care, think again.
According to the Nursing and Midwifery Board of Australia, “’cultural safety’ is as important to quality care as clinical safety”. And there’s no objective test of ‘cultural safety’; it’s determined, so the Board says, by the “recipient of care”. You see, it’s not just what the nurse does that matters but “how a health professional does something”.”
Graeme Haycroft from @NursesPAQ: There's 350,000 nurses and midwives Australia-wide and they're all subject to this code which encourages them to recognise their 'white privilege'.
Graeme has spent a lifetime working in industrial relations and was the man who set up Haycroft Workplace Solutions, leading provider of workplace consulting and management that has nearly 2000 workers on the payroll.
He is chair of the Liberal National Party’s labour market policy committee, active in the HR Nicholls Society, is a regular commentator on labour market issues, and has published his thoughts in such places as the IPA Review, Courier Mail and Online Opinion. But Graeme’s most important contributions have come through what he has done, not what he has written or said.
In the 1990s Graeme famously fought the Australian Workers’ Union to set up sub-contracting for shearers in Charleville, and went on to battle the CMFEU in helping to set up union-free high-rise construction sites. When the Howard government allowed Australian Workplace Agreements (AWAs), Graeme was instrumental in creating the most widely copied template in the country, and his business helped set up about 30,000 agreements.
Lately, Graeme has been working on a exciting new project with the potential to fundamentally change the role and power of unions in this country, while improving services for workers.
He is not waiting for politicians to act; he is changing the system himself… and after years of planning he is finally ready to show us how.
So who is this new Nurses Professional Association of Queensland ?
Queensland Association Services Group QAS Group and Sajen Legal have established a new business model for Employee Associations Queensland Association Services Group (QAS Group), who are the contracted service providers for the NPAQ, in conjunction with Sajen Legal have developed and set up a new association business model.
Working with a small group of dedicated and experienced nurses, they have built in a strict separation between the money earned and spent on the one hand, and the control of the Association on the other.
To launch NPAQ, the QAS Group , have backed the provision of services for ten years under contract. They have provided all of the seed funding for the administrative and legal services including the member Professional Indemnity Insurance policy required of the Association..
Whilst it will be many years before all the seed funding is fully repaid, at the end of our second year, the membership income was sufficient to fund all the running expenses of the NPAQ
” And they quote no party politics “
The NPAQ executive is resolute that there will be no party politics. Every cent of your NPAQ membership money is spent on nurse services and issues
When NACCHO pointed out that NursesPAQ was ” using the definitions of two America right wing commentators to justify mounting a political membership campaign in which you sensationalise and falsely quote out of context aspects of our Indigenous cultural safety in Australia ”
I rang my dad over the weekend. We’d hardly begun yarning before he asked me: “What’s this about white nurses having to apologise to us for being white?”
I could have just said, “Dad, you should know better than to believe what the mainstream media says about us.”
But instead I took the time to explain the truth behind recent misleading media reports on new codes of conduct for nurses and midwives.
Media outlets have aired wrongful claims that the codes would force white nurses to ‘apologise to Indigenous clients for being white’.
The codes do not say that – that idea was invented and then pushed on these media programs.
As Luke Pearson recently wrote for IndigenousX, these stories were not based in facts, but seem to have been driven by the partisan politics of a fringe nursing group, and conservative politicians who have been approached to comment on the wrongful claims.
I took the time to have the conversation with my Dad because it is important people understand how significant these new codes are for efforts to improve the care of our people, hence I thought it important to reach out to the readers of IndigenousX too.
I am sure that some of our nursing and midwifery members and community will be hearing disturbing claims.
Let me be clear, nurses and midwives under the new code do not have to announce their ‘white privilege’ before treating Indigenous clients.
I also had the conversation because, to be honest, I am really proud of these new codes, and not only because the Congress of Aboriginal and Torres Strait Islander Nurses and Midwives (CATSINaM) contributed to their development, which included extensive consultation across nursing and midwifery and at the time no one opposed the inclusion of cultural safety.
We are delighted the Nursing and Midwifery Board of Australia (NMBA) listened to CATSINaM in developing these new codes, and took on board our advice that cultural safety should be recognised as an integral part of ethical and competent professional practice. Further, they cited some of our work at CATSINaM in materials supporting the code.
CATSINaM has been at the forefront of advocating for cultural safety training for health professionals at all levels of health systems in order to improve care for both Indigenous clients and their families. Improving the cultural safety of workplaces is also a vital strategy for improving the recruitment and retention of Indigenous health professionals and staff. We need more of our people in the health system.
Rather than being criticised by sensationalist, inaccurate reports, the NMBA deserves credit for showing leadership in the area of cultural safety. They have set a great example for other health professions and organisations. It wouldn’t be the first time that nurses and midwives have been at the forefront of leading change.
In fact, this is also not the first time this has happened. In many ways, Australia is playing a game of ‘catch up’.
In New Zealand, cultural safety is part of the nursing and midwifery code of conduct and also in the laws that nurses and midwives must follow to be registered to practice. This happened well over 10 years ago because many Maori nurses worked hard for many years to teach their non-Maori colleagues about cultural safety and gain their support so they could provide better care for their people. This is considered completely normal in New Zealand.
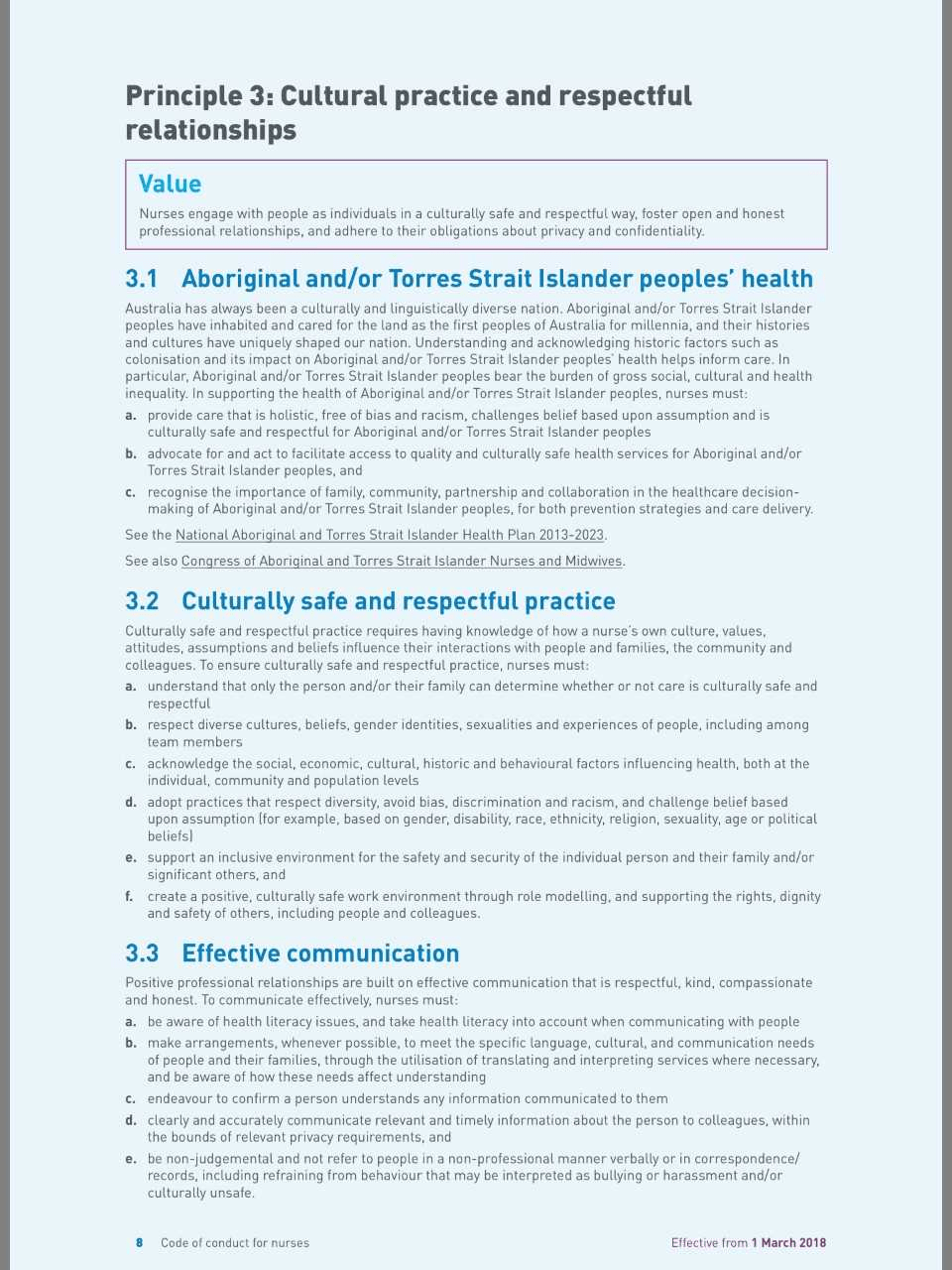
Under the new codes, which took effect on 1 March, nurses and midwives must take responsibility for improving the cultural safety of health services and systems for Aboriginal and Torres Strait Islander clients and colleagues.
They are required to provide care that is “holistic, free of bias and racism”, and to recognise the importance of family, community, partnership and collaboration in the healthcare decision-making of Aboriginal and/or Torres Strait Islander people.
The codes advocate for culturally safe and respectful practice and require nurses to understand how their own culture, values, attitudes, assumptions and beliefs influence their interactions with people and families, the community and colleagues (for more information on our position on Cultural Safety please visit our website).
As part of such reflexive practice, nurses and midwives are encouraged to consider issues, such as white privilege, and how this can affect the assumptions and practices they bring to the care of clients and how they interact with their families. It must be said that privilege has been discussed in Australia for some time – although we are more used to talk about class privilege in Australia – those who have more financial resources compared to those who don’t.
Over time we have recognised there different forms of privilege – men have male privilege in contrast to women. Able-bodied people have able-bodied privilege compared to people living with different types of disabilities. Heterosexual people have heterosexual privilege compared to people who are lesbian, gay, bisexual, transgender, intersex or queer. Not to mention what we have been socialised to believe is normal!
Many people have campaigned for decades to help us learn about these different forms of privilege and do something to change inequity they cause. This has involved education, advocacy, legislation, policies and professional codes of conduct. The acknowledgement of these different forms of privilege and the non-acceptance of biased treatment has resulted in improved circumstances for women, people living with disabilities and lesbian, gay, bisexual, transgender, intersex or queer people. But there is still a long way to go in all of these areas, and especially so where they intersect.
There has been considerable work over the last 20-30 years to talk about white privilege and address the inequity that many white Australians don’t see or realise is there, although Aboriginal and Torres Strait Islander Australians live this every day.
Cultural safety training does include examining how Indigenous people have been locked out of the opportunities that most white people take for granted by past policies and this has resulted in intergenerational exclusion and Indigenous disadvantage. This means that white privilege is one of the areas that people must explore and understand. This is what the codes are asking nurses and midwives to do – to think this through so they do not make incorrect and unhelpful assumptions based on their idea of what is normal for non-Indigenous Australians, particularly white Australians.
A glossary accompanying the new codes cites CATSINaM materials. It identifies that the concept of cultural safety was developed more than 20 years ago in a First Nations’ context (in New Zealand) and holds that the recipient of care – rather than the caregiver – determines whether care is culturally safe. That means you determine if the care you receive is culturally safe.
Instead of providing care regardless of difference, such as when people say ‘I treat everyone the same’, to providing care that takes account of peoples’ unique needs. This includes their cultural needs.
While this is important for Indigenous clients, it also has the potential to improve all clients’ care by encouraging health practitioners to be more reflexive and responsive to the needs of different clients.
Despite what recent headlines might have us believe, there is widespread support for cultural safety’s implementation across the health system.
The National Aboriginal and Torres Strait Islander Health Plan: 2013-2023 (2015) and its associated Implementation Plan (both available here) identify the importance of cultural safety in addressing racism in the health system, and many health services already provide cultural safety training for their staff.
The Australian Nursing and Midwifery Federation, the Australian College of Nursing, the Australian College of Midwives are united with CATSINaM in strongly supporting the guidance around cultural safety in the new codes of conduct.
The Council of Deans of Nursing and Midwifery also considers cultural safety an integral part of competencies for registered nurses and midwives. Providing culturally safe care that is free from racism should be a normal expectation. All health professionals learning about cultural safety and building it into their codes of conduct is a very important step to this becoming a reality. Hence nurses and midwives are currently required to study Aboriginal and Torres Strait Islander health, culture, history, and cultural safety as part of their study programs.
Cultural safety is talked about and implemented in other fields, including education, and family and community services, although people in these fields are still learning about it so it is not always standard practice yet. In fact, CATSINaM recommended cultural safety training for journalists in our submission to the recent Senate Inquiry into the future of public interest journalism, and the latest media fracas indicates just how sorely this is needed.
It is important that we continue these conversations about the importance of cultural safety for healthcare and other systems – they are potentially life-saving.
In response to Graeme Haycroft’s recent comments, we welcome the opportunity to provide further information on how important cultural safety is for improving health outcomes and experiences for Aboriginal and Torres Strait Islander Peoples.
It is clear from the 2018 Closing the Gap Report tabled by Prime Minister Turnbull in February 2018 that Aboriginal and/or Torres Strait Islander Peoples still experience poorer health outcomes than non-Indigenous Australians. It is well understood these inequities are a result of the colonisation process and the many discriminatory policies to which Aboriginal and/or Torres Strait Islander Australians were subjected to, and the ongoing experience of discrimination today.
All healthcare leaders and health professionals have a role to play in closing the gap.
The approach the NMBA has taken for nurses and midwives (the largest workforce in the healthcare system) by setting expectations around culturally safe practice, reflects the current expectations of governments to provide a culturally safe health system. (For more information please see the COAG Health Council 4 August 2017 Communiqué).
Culturally safe and respectful practice is not a new concept. Nurses and midwives are expected to engage with all people as individuals in a culturally safe and respectful way, foster open, honest and compassionate professional relationships, and adhere to their obligations about privacy and confidentiality.
Many health services already provide cultural safety training for their staff. Cultural safety is about the person who is providing care reflecting on their own assumptions and culture in order to work in a genuine partnership with Aboriginal and Torres Strait Islander Peoples.
Nurses and midwives have always had a responsibility to provide care that contributes to the best possible outcome for the person/woman they are caring for. They need to work in partnership with that person/woman to do so. The principle of cultural safety in the new Code of conduct for nurses and Code of conduct for midwives (the codes) provides simple, common sense guidance on how to work in a partnership with Aboriginal and Torres Strait Islander Peoples. The codes do not require nurses or midwives to declare or apologise for white privilege.
The guidance around cultural safety in the codes sets out clearly the behaviours that are expected of nurses and midwives, and the standard of conduct that patients and their families can expect. It is vital guidance for improving health outcomes and experiences for Aboriginal and Torres Strait Islander Peoples.
The codes were developed through an evidence-based and extensive consultation process conducted over a two-year period. Their development included literature reviews to ensure they were based on the best available international and Australian evidence, as well as an analysis of complaints about the conduct of nurses and midwives to ensure they were meeting the public’s needs.
The consultation and input from the public and professions included working groups, focus groups and preliminary and public consultation. The public consultation phase included a campaign to encourage nurses and midwives to provide feedback.
The Australian Nursing and Midwifery Federation, the Australian College of Nursing, the Australian College of Midwives and the Congress of Aboriginal and Torres Strait Islander Nurses and Midwives all participated in each stage of the development and consultation of the new codes. The organisations strongly support the guidance around cultural safety in the codes for nurses and midwives.
Lynette Cusack
Chair Nursing and Midwifery Board of Australia
Ann Kinnear
CEO
Australian College of Midwives (ACM)
Kylie Ward
CEO
Australian College of Nursing (ACN)
Janine Mohamed
CEO
Congress of Aboriginal and Torres Strait Islander Nurses
and Midwives
Annie Butler
A/Federal Secretary Australian Nursing and Midwifery
Federation
For more information:
Part 3 QNMU Secretary Beth Mohle has issued a statement clarifying misleading comments in the media over the weekend around the NMBA’s new Codes of Conduct for nurses and midwives.
I was stunned to read businessman Graeme Haycroft’s comments regarding nurses and indigenous Australians on the weekend, as part of his criticism of the new NMBA Codes and the term cultural safety which is defined in a glossary connected to the codes.
These codes were the subject of lengthy consultations with the professions of nursing and midwifery and other stakeholders including community representatives. This review was comprehensive and evidenced-based. Our union and our national body the Australian Nursing Midwifery Federation (ANMF) were active participants in these consultations.
The codes, written by nurses and midwives for nurses and midwives, seek to ensure the individual needs and backgrounds of each patient are taken into account during treatment.
There’s no doubt cultural factors, including how a patient feels while within the health system, can impact wellbeing. For example, culture and background often determine how a patient would prefer to give birth or pass away.
Every day, nurses and midwives consider a range of complex factors, including a patient’s background and culture to determine the best treatment. These codes simply articulate what is required to support safe nursing and midwifery practice for all.
Mr Haycroft stated that the new code “has been sponsored and supported by the QNU to promote its party political social policy.”
This statement is disturbing on a number of levels. The Queensland Nurses and Midwives’ Union (QNMU) has repeatedly refuted Mr Haycroft’s allegations we donate to political parties. We do not. Nor are we affiliated with any political party. Yet Mr Haycroft continues to repeat these claims.
Secondly, this statement demonstrates a failure to understand the basics. It is the Nursing and Midwifery Board of Australia (NMBA) that regulates the practice of nurses and midwives through its standards, codes and guidelines.
The QNMU actively participates in NMBA consultations and represents the interests of our members individually and collectively. However, the new codes have not been “sponsored” by our union.
As a not-for-profit organisation run by nurses and midwives for nurses and midwives, the QNMU will remain steadfastly focused on advancing the values and interests of our members and the safety of those in their care. We will not be diverted by the political or business agendas of others.
But first tonight, the contentious new code telling nurses to say “sorry for being white” when treating their Indigenous patients.
That’s how Today Tonight Adelaide began last night.
It continued:
“Now, it’s the latest in a string of politically correct changes for the health industry, but this one has led to calls for the Nursing Board boss to resign.”
It was followed by a five minute story with the new code being condemned by someone you’ve probably never heard of, Graeme Haycroft, explaining that:
“According to how the code is written, the white nurse would come in and say, ‘before I deal with you, I have to acknowledge to you that I have certain privileges that you don’t have” followed by Cory Bernardi calling it divisive.
It goes on in this vein for a full five minutes before it cuts back to the presenter, who finally says, “The Nursing and Midwifery Board has told us that the code was drafted in consultation with Aboriginal groups and has been taken out of context as it’s not a requirement for health workers to declare or apologise for white privilege”.
And just to reinforce that point, the entire premise for the segment was false. There is no requirement for nurses to apologise for being white, which would be very awkward for the more the more than 1500 Indigenous nurses across Australia, and the countless others who also aren’t white to begin with. But, even for the nurses who are – THERE IS NO REQUIREMENT FOR THEM TO APOLOGISE FOR BEING WHITE.
So, why on Earth would Today Tonight run such a story?
Why would they base a story off the demonstrably false allegations of this Graeme Haycroft person?
“A member of the National Party and the H.R. Nicholls Society, he (Mr Haycroft) boasts that, because of a tussle he had with the Australian Workers Union 15 years ago, the union does not have a single member shearing sheep in south-western Queensland today.
Now he runs a labour hire firm with a thriving sideline in moving small-business employees off awards and collective agreements and onto the Federal Government’s preferred individual contracts, Australian Workplace Agreements.
…Mr Haycroft’s business stands out because he is targeting lower-skilled, lower-paid workers, often with poor English – the people unions say have much to fear from individual contracts.”
Cut back to 2018, and Graeme Haycroft now runs the Nurses Professional Association of Queensland, which promotes itself as an alternative to the Qld Nurses Union.
So, a man with a long history of fighting Unions, who ‘saved’ the mushroom farming business by showing businesses how to move “small-business employees off awards and collective agreements and onto the Federal Government’s preferred individual contracts, Australian Workplace Agreements.”
According to the 2005 article, “Mr Haycroft said workers had been more than happy to sign on, most with their penalty rates, holiday pay and other conditions being rolled into a flat rate.”
“However, [there is always a ‘however’], Mr Haycroft was stripped of his preferred provider status with the Office of the Employment Advocate on Thursday, after a Sydney picker, Carmen Walacz Vel Walewska, said she was sacked after she contacted the Australian Workers Union for advice on AWAs.”
With that track record, it’s hard to imagine why nurses would want to leave their current union in favour of his ‘professional association’.
It seems as though, once again, Indigenous people have become a political football and a convenient scapegoat for issues that have nothing to do with us.
Queensland has a long history of political success found through anti-Aboriginal sentiment, so what better way to undermine a Union and recruit new members to a professional association than to accuse the Union of ‘racism against white people’ and ‘political correctness gone made’ by spreading the blatantly false and misleading accusation that white nurses now have to apologise to Aboriginal people for being white?
And just like Dick Smith’s anti-immigration campaign, Blair Cottrell’s anti-African ‘community safety group’, and Prue McSween’s call for a new Stolen Generation, it seems Channel 7 is always more than happy to ignore the facts and sensationalise issues about race and racism.
There is always one more thing.
We, and others, will soon publish articles explaining what the Code of Conduct actually calls for, and explain why cultural competence and cultural safety are important (editor’s note: we did, here’s one of them), but I can’t help but be reminded of this quote from Toni Morrison:
“The function, the very serious function of racism is distraction. It keeps you from doing your work. It keeps you explaining, over and over again, your reason for being. Somebody says you have no language and you spend twenty years proving that you do. Somebody says your head isn’t shaped properly so you have scientists working on the fact that it is. Somebody says you have no art, so you dredge that up. Somebody says you have no kingdoms, so you dredge that up. None of this is necessary. There will always be one more thing.”
So, instead of working on the very real business of ensuring best practice within the nursing industry, our Indigenous experts in this area will have to take a few days away from this important work to explain that no one is asking for white nurses to apologise for being white.
Just like we have to explain that not all Aboriginal parents abuse their children, or that we don’t want to steal white people’s backyards, or that we had (and have) science, or that Australia wasn’t Terra Nullius, or, as Malcolm Turnbull suggested last year, that acknowledging Indigenous history and addressing the issue of colonial statues and place names across Australia is not a “Stalinist exercise of trying to wipe out or obliterate or blank out parts of our history”.
So long as Australian media and politics finds value, profit and opportunity in promoting racism, there will always be one more thing.
So, I might as well clear up a few others while I’m here, and empty a few more buckets out of the endless ocean of racist misinformation.
Child abuse isn’t a ‘cultural’ thing.
Police are not scared to arrest Aboriginal people out of fear of being called racist.
We don’t get free houses.
Aboriginal people using white ochre on their faces in dance and ceremony is not the same thing as white people dressing up in blackface.
We don’t get free university.
The Voice to Parliament is not a third chamber of parliament.
We are not the problem.
Anything else?
We aren’t vampires?
We don’t shoot laser beams out of our eyes?
We aren’t secretly developing a perpetual motion machine that runs on white tears?
I’m sure I, and countless others, will undoubtedly need to keep adding to this list because, as Toni Morrison tells us, there will always be one more thing.
I’VE seen a lot of crazy political correctness in my time but the new Nurses’ Code of Conduct is right up there with the worst of it.
If you thought nursing was about quality health care, think again.
According to the Nursing and Midwifery Board of Australia, “’cultural safety’ is as important to quality care as clinical safety”. And there’s no objective test of ‘cultural safety’; it’s determined, so the Board says, by the “recipient of care”. You see, it’s not just what the nurse does that matters but “how a health professional does something”.
According to the commissars at the Board, “’cultural safety’ represents a key philosophical shift from providing care regardless of difference, to care that takes account of peoples’ unique needs”.
Changes to the Code mark a philosophical shift in the industry. (Pic: supplied)
What this means is that nurses are no longer required to be colourblind; instead, they must see colour and treat patients differently because of it.
According to the Code, the Board declares, “cultural safety provides a decolonising model of practice based on dialogue, communication, power sharing and negotiation and the acknowledgment of white privilege” (no, I am not making this up — it’s on page 15 of the Code effective 1 March 2018).
The Board decrees that “non-indigenous nurses must address how they create a culturally safe work environment that is free of racism”. Now I know many nurses, including my sister who has spent 20 years working selflessly in indigenous communities, and the idea that they are subtly racist or even insensitive to their patients’ needs is as offensive as the leftist sanctimony that has infected their professional body.
The changes to the Code were endorsed by COAG. (Pic: iStock)
When a body representing some nurses had the temerity to complain about this, Board Chair Associate Professor Lynette Cusack disdainfully replied that it had been endorsed by COAG.
Well, I checked with the Federal health minister Greg Hunt and that’s not accurate. The Minister’s own advice from his Chief Nursing Officer and health department noted that “while the Commonwealth Department of Health provided feedback in the public consultation process, the final changes to cultural safety were made after (this) process. The Department did not see the final version until it was publicly released in March 2018.”
Greg Hunt is one of the smartest politicians I know; I didn’t think he would have let this get through, had he known about it, without a fight.
” In the fifth part of a series focusing on the coming third edition of the ‘National guide to a preventive health assessment for Aboriginal and Torres Strait Islander people’, newsGP looks at Aboriginal and Torres Strait Islander peoples’ sexual health and prevention from blood-borne viruses.”
The third edition of the National Guide will be launched next Wednesday 28 March by Minister Wyatt at Parliament House Canberrasee content details Part 2 below
The NACCHO/RACGP National Guide is a resource created for primary healthcare practitioners to help them deliver best practice preventive healthcare to Aboriginal and Torres Strait Islander people anywhere in Australia.
The National Guide is user-friendly with information that is accurate and relevant to Aboriginal and Torres Strait Islander people and communities. It is supported by evidence-based recommendations, good practice points, and child, youth and adult lifecycle wall charts with age-specific recommendations.
New topics 3 edition :
• Fetal alcohol spectrum disorder
• Interventions to prevent child maltreatment – optimising child health and wellbeing
• Antenatal care section is now expanded
• Family abuse and violence
• Lung cancer
• Young people lifecycle summary wall chart to complement the existing child and adult charts.
Part 1 : Sexual health education for Aboriginal and Torres Strait Islander peoples
Edited by Morgan Liotta
The National Guide details several resources that aim to empower Aboriginal and Torres Strait Islander communities through greater levels of sexual health education.
Sexually transmitted infection (STI) and blood-borne virus (BBV) rates within Aboriginal and Torres Strait Islander populations can often be difficult to identify and diagnose, due to certain cultural beliefs and a potential lack of access to appropriate healthcare in remote areas. But education and culturally appropriate primary healthcare play an essential role in helping to increase diagnosis these communities
The National Aboriginal Community Controlled Health Organisation’s (NACCHO) and the RACGP’s National guide to a preventive health assessment for Aboriginal and Torres Strait Islander people (National Guide) states that the prevalence and incidence of some STIs can also be challenging to estimate accurately due to under-identification of Aboriginal and/or Torres Strait Islander status, but that rates are increasing.
The National Guide advocates for interventions by healthcare professionals to help decrease rates of STIs and BBVs in Aboriginal and Torres Strait Islander communities. Routine screening, education on and accessibility of condoms, hepatitis B and human papillomavirus (HPV) immunisation programs, and needle and syringe exchange programs, can all contribute to early diagnoses and prevention of STIs and BBVs, as well as appropriate management for those diagnosed with infection.
Aboriginal and Torres Strait Islander people are over-represented in prison populations and have high rates of receptive sharing of syringes, both risk factors for acquiring hepatitis C. As a consequence, the hepatitis C notification rate among Aboriginal and Torres Strait Islander people has increased by more than 20% between 2012–16, while remaining stable in non-Indigenous Australians. With new, effective treatments now available for hepatitis C, eliminating the stigma associated with the infection is a crucial strategy.
Recent research reveals that gonorrhoea notifications are seven times more common among Aboriginal and Torres Strait Islander people than for non-Indigenous Australians. The chlamydia notification rate in major cities was found to be nearly three times as high among Aboriginal and Torres Strait Islander people than non-Indigenous Australians, increasing to five times higher in remote areas.
In addition, rates of syphilis are again increasing in Aboriginal and Torres Strait Islander communities, after declining up to 2010.
The National Guide reports that rates of HIV were more than two times higher for Aboriginal and Torres Strait Islander peoples than for non-Indigenous Australians in 2015, and that infectious syphilis notifications have increased significantly due to a 2015 outbreak in Far North Queensland. Current syphilis infection in northern Australia is considered ‘out of control’ in Aboriginal and Torres Strait Islander healthcare organisations.
One example of safe-sex education is the Condom tree program in Western Australia, which aims to reduce cost barriers and feelings of shame and embarrassment by providing free condoms in local communities.
The Department of Health recently released a series of videos voiced by Aboriginal and Torres Strait Islander people to help promote STI prevention in their communities. Initiatives such as these videos are designed to help reduce feelings of shame or stigma Aboriginal and Torres Strait Islander people may have attached to STIs and/or BBVs.
A diverse range of support for Aboriginal and Torres Strait Islander peoples and healthcare workers, including a comprehensive HIV resource, is available for communities throughout Australia.
The National Guide details more resources, with the aim of empowering Aboriginal and Torres Strait Islander communities through greater levels of sexual health education and the provision of high-quality culturally appropriate primary care.
The National Guide covers further information on sexual health in the following chapters:
Sexual health and blood-borne viruses
Antenatal care
The health of young people
Alcohol
Family abuse and violence
The National Guide was conceived by the National Aboriginal Community Controlled Health Organisation (NACCHO) in 2001, and is now in its third edition being developed in partnership by NACCHO and The Royal Australian College of General Practitioners (RACGP).
Part 2 What is the National Guide? Edition 3
Who is it for?
All health professionals delivering primary healthcare for the benefit of Aboriginal and Torres Strait Islander people.
Why use it?
• To help prevent disease, detect early and unrecognised disease, promote health, and consider broader social interventions, while allowing for local and regional variations.
• For evidence-based recommendations and good practice points.
• For the child, young people and adult lifecycle wall charts with age-specific recommendations.
• For the resource lists.
When will it be published?
The third edition of the National Guide and following associated resources will be available in early 2018:
• National Guide website – improved design and usability
• National Guide recommendations – limited print run for ACCHSs
• National Guide evidence base – downloadable PDF.
What’s happening in 2018 to accompany the launch of the
National Guide?
• The third edition of the National Guide will be distributed to NACCHO Affiliates and health services.
• NACCHO and RACGP will be hosting workshops across Australia to support implementation of the National Guide.
What’s new in the third edition?
New topics:
• Fetal alcohol spectrum disorder
• Interventions to prevent child maltreatment – optimising child health and wellbeing
• Antenatal care section is now expanded
• Family abuse and violence
• Lung cancer
• Young people lifecycle summary wall chart to complement the existing child and adult charts.
How to access the National Guide:
The third edition of the National Guide will be March 28
Free to download on the RACGP website and the NACCHO website:
1.VIC : Essendon Football Club and The Long Walk partners with Victorian Aboriginal Health Services (VAHS) to promote Deadly Choices
2.NSW :Awabakal opened a new Community Clinic to mark National Close the Gap Day
3.WA : The AHCWA team took action to raise awareness of National Close the Gap Day 2018!
4.NT : Mobile health lab expands educational offering through Heart Foundation partnership
5.ACT : Winnunga ACCHO Download monthly News from CEO Julie Tongs
6.QLD : Apunipima ACCHO Closing the Gap on health inequality for Indigenous mothers and babies in Cape York
7. Tas: TAC : The Tasmanian Aboriginal community gathered in the North-West last weekend for an annual celebration of Aboriginal culture, heritage and land ownership.
Wednesday by 4.30 pm for publication each Thursday
1.VIC : Essendon Football Club and The Long Walk partners with Victorian Aboriginal Health Services (VAHS) to promote Deadly Choices
“We’re proud and pleased to partner with another urban Community Controlled Health Service (VAHS) to deliver Deadly Choices to their communities. Programs like Deadly Choices demonstrate that the solution to improving Indigenous health and well-being is within Aboriginal and Torres Strait Islander communities,”
CEO of the Institute for Urban Indigenous Health, Adrian Carson, is excited to see Essendon and VAHS rolling out Deadly Choices in their region.
Essendon Football Club and The Long Walk are proud to announce they have partnered with Victorian Aboriginal Health Services (VAHS) to promote the Aboriginal and Torres Strait Islander preventative health campaign, Deadly Choices.
A social marketing campaign developed by the Institute for Urban Indigenous Health (IUIH), Deadly Choices aims to empower Aboriginal and Torres Strait Islander people to make healthy choices for themselves and their families, with a specific focus on:
Quitting smoking
Eating a healthy diet
Exercising daily
Accessing their local Community-Controlled Health Service for an annual ‘Health Check’
The Club will work closely with VAHS and IUIH in order to encourage more Aboriginal and Torres Strait Islander people to make Deadly Choices.
General Manager of The Long Walk and Indigenous Affairs, Leanne Brooke, said Essendon is the first AFL Club in Victoria to get behind Deadly Choices.
“Essendon and The Long Walk are proud to support Deadly Choices, and we look forward to working closely with VAHS and IUIH to improve health outcomes for Aboriginal and Torres Strait Islander people,” Brooke said.
“Essendon’s strong following, and our long and proud connection to Aboriginal and Torres Strait Islander communities, will not only help us promote the importance of making Deadly Choices in the North of Melbourne but right across Australia.
“Partnering with VAHS using the Deadly Choices preventative health campaign reinforces Essendon and The Long Walk’s ongoing commitment to celebrating, educating and empowering Australia’s first nation’s people.”
As part of the new partnership, Anthony McDonald-Tipungwuti, Joe Daniher and Michael Hurley were unveiled as the Club’s Deadly Choices Ambassadors.
Today the trio joined their teammates in showing off the new Essendon themed Deadly Choices t-shirts, which participants receive after having an annual health check.
CEO of VAHS, Michael Graham, said the new partnership would raise vital awareness about the importance of good health for Aboriginal and Torres Strait Islander people.
“For VAHS, Deadly Choices as a marketing tool is a ‘game- changer’ for the long term health and well-being of our people,” Mr Graham said.
“When we get on the front foot and have people informed about their health status and support them to take control with Deadly Choices, then we are heading in the right direction.”
CEO of the Institute for Urban Indigenous Health, Adrian Carson, is excited to see Essendon and VAHS rolling out Deadly Choices in their region.
“We’re proud and pleased to partner with another urban Community Controlled Health Service (VAHS) to deliver Deadly Choices to their communities. Programs like Deadly Choices demonstrate that the solution to improving Indigenous health and well-being is within Aboriginal and Torres Strait Islander communities,” Carson said.
“Essendon players will promote the preventative health messaging that will attract even more clients to VAHS health clinics, to make their health a priority.”
To find out where your nearest VAHS clinic is, click here.
2.NSW :Awabakal opened a new Community Clinic to mark National Close the Gap Day
On Thursday 15 March, Aboriginal organisation Awabakal opened a new Community Clinic in Raymond Terrace to mark National Close the Gap Day.
This new Clinic will be the start of an expansion for Awabakal as they work to meet the region’s demand for Aboriginal health and community services and to assist in addressing the serious issue of the disparity in life expectancy between Indigenous and non-Indigenous Australians. In addition to the new Raymond Terrace site, another Clinic will open in Cardiff in April and there are plans to service an additional two communities with their mobile outreach clinics.
Awabakal’s Chief Executive Officer, Raylene Gordon is proud of the organisation’s growth and the support they have had from the community.
“It’s wonderful to see our community growing as people engage with our services. To now have the opportunity to take these services to a wider territory takes us a step closer to closing the gap,” says Raylene.
=“We are always aiming to lead the way in delivering culturally appropriate health and wellbeing services to our people. The Raymond Terrace site is exciting because it is a partnership with a local Aboriginal organisation, Wahroonga.
Awabakal’s new Clinic will operate to provide additional access to services already delivered by Awabakal Medical Service in Hamilton which currently provides primary health care, advocacy, social and emotional support to Aboriginal families in the Newcastle area.
In additional to growing their geographical reach, Awabakal has also recently expanded their services by becoming a registered provider of the National Disability Insurance Scheme (NDIS). They are also currently in the process of developing new Youth programs to continue to work towards closing the gap in life expectancy by providing better services and opportunities for Aboriginal people from a young age.
With more than 40 years behind them as an Aboriginal managed not-for-profit organisation, Awabakal continues to set the standard for Indigenous health services that both honour the Aboriginal culture whilst opening the possibilities for greater equality in the health and wellbeing of all Australians.
Visit www.awabakal.org for more information about Awabakal’s services
3.WA : The AHCWA team took action to raise awareness of National Close the Gap Day 2018!
The Close the Gap campaign calls on governments to take real, measurable action to achieve Indigenous health equality by 2030
4.NT : Mobile health lab expands educational offering through Heart Foundation partnership
People living in remote Northern Territory communities will benefit from an expanded health education offering through a partnership between Menzies School of Health Research (Menzies) and the Heart Foundation.
This year, Menzies’ mobile health laboratory HealthLAB will be delivering the Heart Foundation’s LiveLighter program to five remote communities in the Top End and three communities in Central Australia.
Associate Professor Heidi Smith-Vaughan, HealthLAB director, said the team was excited to show people living in remote Australia ways to lower their risk of developing chronic diseases by delivering hands-on health promotion.
“LiveLighter is a fantastic public education campaign. It aligns with the aims of HealthLAB, which is promoting positive health behaviours and empowering people to reduce the risks of developing health issues later in life for themselves and future generations,” Assoc Prof Smith-Vaughan said.
The LiveLighter program aims to encourage Australian adults to lead healthier lifestyles by making simple changes to what they eat and drink, and by being more active.
HealthLAB uses the latest health technology to measure participants’ health and inform them about the impacts of smoking, alcohol misuse and diet, which can increase the risk of long-term diseases such as diabetes, cancer, kidney disease, obesity and heart disease.
HealthLAB stations are operated by dieticians, sonographers, clinical professionals and scientists who provide education and measure physical health through body impedance, blood pressure, carbon dioxide analyser, and upper body strength, among others.
Heart Foundation Northern Territory CEO, Simon Dixon, said the Heart Foundation was delighted to be partnering with Menzies to deliver HealthLAB to communities in the Territory.
“Healthy lifestyles lead to healthy hearts,” said Mr Dixon.
“The LiveLighter program has successfully educated thousands of Australians about the importance of healthy nutrition and activity,” he said.
“Now with the involvement of HealthLAB we will be able to spread this message to a really important audience in remote communities as well.”
The first HealthLAB and LiveLighter program was delivered in Maningrida on Close the Gap Day, Thursday, 15 March 2018. The team also set up at the Tiwi Islands AFL Grand Final on Sunday, 18 March 2018.
5.ACT : Winnunga ACCHO Download monthly News from CEO Julie Tongs
I was very pleased, in late February to again welcome Minister for Health Ms Meegan Fitzharris and Minister for Community Services Ms Rachel Stephen-Smith to Winnunga AHCS. I am genuinely grateful for the interest which both Ministers are showing in Winnunga AHCS and the Aboriginal and Torres Strait Islander community.
The primary purpose of the meeting was to update the Ministers on initial concept and design work which Winnunga AHCS has commissioned Judd Consulting to undertake in respect of the proposed new health and community services facility. A number of issues were covered during the discussion on plans for the new building. These included issues such as timing, project management, funding model, lease arrangements, ownership, design, construction and parking.
This is an incredibly exciting and important project for Winnunga AHCS and all of its clients and I am grateful for the collaborative approach which Minister Fitzharris, in particular, has adopted.
At the meeting with the Ministers we also discussed the plan announced recently by the Government to establish an Aboriginal and Torres Strait Islander Centre of Excellence in Health at the Canberra Hospital. I expressed some surprise that neither the reason nor rationale for the creation of the Centre of Excellence in Aboriginal and Torres Strait Islander Health had been conveyed to either me or anyone at Winnunga AHCS. I explained it was not clear what role the Centre would play and how it would relate to Winnunga AHCS – the first choice for health care for the majority of Canberra’s Aboriginal community. The Minister advised that while she had understood that Winnunga AHCS had been consulted about the proposal she was most concerned that that was not the case. I await with interest an explanation of what it is that the proposed Centre will do.
I also discussed with the Ministers my concerns about the continuing delay in finalising the tender process for the return of Boomanulla Oval to Aboriginal control and management.
The meeting with Ms Fitzharris and Ms Stephen-Smith was open and constructive and I look forward to their continued interest in, and support of the local Aboriginal and Torres Strait Islander community.
6.QLD : Apunipima ACCHO Closing the Gap on health inequality for Indigenous mothers and babies in Cape York
Apunipima Cape York Health Council announces a new project to address the health inequality of Indigenous mothers and babies in Cape York.
Families in remote Cape York communities will benefit from a new project being undertaken by Apunipima Cape York Health Council to improve nutrition before, during and after pregnancy.
Apunipima has been awarded funding from Northern Queensland Primary Health Network (NQPHN) to deliver the Optimal Infant Nutrition for Cape York Mums Project.
The project will build upon Apunipima’s award-winning Baby One Program and further develop a suite of tools, workshops and activities around nutrition for mothers and infants to improve long-term health and wellness outcomes.
Population Health and Research Team Leader Melinda Hammond said it is well known that underlying poor nutrition is a major contributing factor to the higher burden of disease experienced by Aboriginal and Torres Strait Islander people compared with other Australians.
“We know that improving health and life expectancy starts early in life. The healthier a pregnancy is, the healthier the child will be and the better they will learn and grow.” said Ms Hammond.
NQPHN Chief Executive Officer John Gregg said improving Aboriginal and Torres Strait Islander health by closing the gap is a priority area of NQPHN.
“This partnership with Apunipima will assist in education for families that may otherwise be out of reach for many within Cape York communities.
“We are proud to be a part of this program, as we continuously work towards helping northern Queenslanders to live happier, healthier, and longer lives.”
Aboriginal women have an increased risk of having low birthweight babies and complications of anaemia, poor nutrition and there are high rates of smoking and chronic disease during pregnancy. This increasing risk of adverse health outcomes for the mother and baby. Poor nutrition before, during and after pregnancy and during the first few years of life can result in chronic disease later in life. Preventing this starts with healthy mothers, babies and children.
The project will be run over the next two years and will initially focus on two Cape York communities. Apunipima will be working in partnership with researchers at James Cook University, Monash University and Menzies School of Health Research to ensure robust evaluation of all the project activities is shared widely.
7. Tas:TAC :The Tasmanian Aboriginal community gathered in the North-West last weekend for an annual celebration of Aboriginal culture, heritage and land ownership.
The three-day camping event was held at Preminghana, a property north of Arthur River that was handed back to the Aboriginal community in 1995.
Scott Wells of Wynyard entertains campers with music. Picture: Supplied
The Preminghana Camp was organised by the Tasmanian Aboriginal Centre and featured cultural activities such as walks on country, kelp basket making, traditional language activities, storytelling and games.
CEREMONY: Brenton Brown of Burnie does a Cleansing Dance while Launceston boys Calvin Riley and J’Kobi Hughes beat clap sticks. Picture: Supplied
TAC North-West regional manager Lisa Coulson said there was “a real sense of community and cultural connectedness” among the 170 people who attended.
Ms Coulson said the camp also provided a chance for family and friends to catch up.
“It was a great opportunity to get kids and their families out of the cities and into their natural environment on their land,” she said.
The TAC also ran workshops on protective behaviours and strategies to keep young people safe, updated the community about land management efforts at Preminghana and had experts on nutrition and quitting smoking on hand.
The annual camp was started in 1991 and moved to Preminghana in 1995.
Aboriginal community members from around Tasmania enjoy cultural activities at the preminghana Camp.
8.SA :SA’s biggest Closing the Gap Day
11am – 3pm
Thursday 22 March 2018
Adelaide Showground, Ridley CentreJoin us for SA’s biggest Closing the Gap Day at the Adelaide Showground.
Closing the Gap Day is a FREE all-ages event which aims to bring together people from the Aboriginal and Torres Strait Islander community to share information and take meaningful action in support of achieving Indigenous health equality by 2030.…FEATURING MUSIC BY NANCY BATES & ELLIE LOVE GROVE
MC SHELLEY WARE | COMEDIAN JOSHUA WARRIOR
DELICIOUS LUNCH | FREE HEALTH CHECKS | HENNA TATTOOS | NGANGKARI TRADITIONAL HEALERS | SA METROPOLITAN FIRE SERVICE TRUCKS | REPTILE ZOO | JUMPING CASTLE & MANY MORE FUN ACTIVITIES FOR KIDSSee More
“As the only Academic Health Science Centre in Australia with a primary focus on Aboriginal and remote health, we are pleased that Minister Hunt is leading on the front foot with an announcement such as this.
It’s especially pleasing that this is happening just as we are about to engage with a wide consultation between our members over health research priorities in Central Australia in the coming years—this three year commitment allows us to do this with confidence.
The Centre is already working in key areas such as endemic HTLV-1 infection, exploring the complex interplay between communicable and chronic disease as well as exploring the capacity of the primary health care sector to reduce avoidable hospitalisations,”
The Chairperson of the Central Australia Academic Health Science Centre [CA AHSC] John Paterson has welcomed the commitment over three years of significant research funding to the Centre by Federal Health Minister Greg Hunt.
“Research projects that will be supported will emphasise those based on community need and initiative especially as expressed by the Aboriginal partner organisations, though this will not necessarily preclude externally identified needs.
In any case, we will focus on comprehensive approaches to consultation and participation in the ethical design of research projects, the carriage of the research, and the rapid implementation of positive research results.
A key activity will be that of building future leaders in the Aboriginal research workforce. We have already started this critical work with the first meeting of a network of more than 15 Aboriginal researchers in Central Australia.”
A health research partnership benefitting Warumungu, Arrernte (Eastern), Pintupi, Pitjantjatjarra, Arrernte (Central), Yankunytjarra, Luritja, Arrernte (Western), Warlpiri, Anmatyere, Ngaanyatjarra, Kaytetye and Alyawarre speakers across Central Australia
Press Release : Medical research to uncover better treatment for Indigenous Australians
The Turnbull Government will invest more than $6 million in a health science centre in Alice Springs which is focused on addressing health challenges faced by Indigenous Australians.
The Central Australia Academic Health Science Centre will receive $6.1 million over three years from the Medical Research Future Fund (MRFF).
This funding will support better treatment and diagnosis of health challenges experienced by Indigenous Australians.
The Centre brings together top researchers, medical experts and local communities to look at ways to improve healthcare options for the specific health challenges facing Indigenous Australians.
The Central Australia Academic Health Science Centre is the first Aboriginal-led collaboration of its kind and demonstrates the importance of Aboriginal community leadership in research and health improvement.
These projects will directly benefit regional and remote Aboriginal communities and it is our hope that medical research will help in closing the gap on disadvantage.
The first priority project that will be supported through the Central Australia Academic Health Science Centre will be a study into addressing HTLV-1.
Additional areas that will be considered by the Centre include addressing research into ear and eye health, renal health and dialysis, children and maternity health in Indigenous communities.
Indigenous health is one of the Turnbull Government’s fundamental priorities and while progress has been made on some key indicators, with male and female life expectancy increasing and child mortality and smoking rates decreasing, more needs to be done.
Today I am also pleased to announce more than $740,000 of MRFF funding for University of Queensland researchers to undertake a world-first project, in collaboration with Aboriginal communities, to find ways to improve Aboriginal food security and dietary intake in cities and remote areas.
Poor diet and food insecurity are major contributors to the excess mortality and morbidity suffered by Aboriginal and Torres Strait Islander people in Australia.
The Turnbull Government is committed to improving the health services for Indigenous Australians and we will continue to invest in better treatment, care and medical research.
1.1 : National : Close the Gap Day: a greater role for Aboriginal community controlled health services essential
1.2 : Ten Close the Gap reasons Aboriginal Community Controlled Health Services are more than just another health service.
2.1 NSW : Sydney Close the Gap Picnic Breakfast event Surry Hills event.
2.2: NSW : Awabakal ACCHO Close the Gap event : Expanding services to the Port Stephens community.
2.3: NSW : Ready Mob and Galambila help Close the Gap at Bowraville Indigenous Health Workforce Expo
3.1 NT : Danila Dilba ACCHO Close the Gap event Darwin
3.2 NT : Congress Alice Springs and CASSE Close the Gap _- Aboriginal Male Health
4.WA AHCWA is hosting a Close the Gap Family Festival!
6.1 : QLD ATSICHS Brisbane team helps to Close the Gap at the women’s fun run
6.2 QLD : Telehealth closes the gap on Indigenous health in Queensland
7. Vic : VAHS is holding an event /Health checks for Closing the Gap Day.
8. SA : Port Power and Deadly Choices support Aboriginal Health checks to Close the Gap
9.Tas: Close the gap Events see link below
1.National : Close the Gap Day: a greater role for Aboriginal community controlled health services essential
Close the Gap Day is a day to acknowledge the critical role Aboriginal medical services and health professionals must play in turning around the significant health gap between Aboriginal and Torres Strait Islander people, the National Aboriginal Community Controlled Health Organisation said today.
After a decade of the Close the Gap campaign, programs and projects managed by Aboriginal services on the ground in local communities are the only model proven to be making inroads in closing the Indigenous health gap.
The evidence tells us that Aboriginal people respond best to health care provided by Aboriginal people or controlled by the Aboriginal community.
At least one-third of the health gap can be attributed to the social and cultural determinants of health.
If we are serious about improving health outcomes for Aboriginal people, governments at all levels must do more to join the dots between education, housing, employment and other determinants and make sure that Indigenous led solutions are at the centre of strategies that make those links.”
10 reasons Aboriginal Community Controlled Health Services are more than just another health service.
Download the 10 Key ACCHO facts with graphics and references
1.NACCHO puts Aboriginal health in Aboriginal hands
See NACCHO TV
2.We are around for the long haul — commitment and continuity are required to close the gap
Our first members have been around since the very early 1970s. Our roots are deep. We have endured as a high quality, clinically accredited community controlled service for over forty years. As the health system becomes more complex, the role of our services becomes even more critical. The Indigenous population is also increasing rapidly, yet funding levels have not kept pace with demand.
3.We punch above our weight:
Aboriginal controlled health services provide about three million episodes of care each year for about 350,000 people. In very remote areas, our services provided about one million episodes of care in 2015-16.1
4.Our customers trust us with their health
Our services build ongoing relationships to give continuity of care so that chronic conditions are managed and preventative health care can be effectively targeted. Studies have shown that Aboriginal controlled health services are 23% better at attracting and retaining Aboriginal clients than mainstream providers.2 Through local engagement and a proven service delivery model, our clients ‘stick’. The cultural safety in which we provide our services is a key factor of our success.
More people are using Aboriginal controlled health services. It is reported that in the 24 months to June 2015, our services increased their primary health care services, with the total number of clients rising by 8% (from 316,269 to 340,299).3 A map showing the footprint of our clients is attached.
5.We are proven to be clinically effective
As recently reported in the Australian Health Review (March 2017), we are more effective than other health services at improving Indigenous health.4 Our services specialize in providing comprehensive primary care consistent with our clients’ needs.
This includes: home and site visits; provision of medical, public health and health promotion services; allied health, nursing services; assistance with making appointments and transport; help accessing child care or dealing with the justice system; drug and alcohol services; and providing help with income support. This is funded by both State and Australian Governments.
6.We provide value for money
Aboriginal controlled health services are cost-effective. Our activities result in greater health benefits per dollar spent; measured at a value of $1.19:$1. The lifetime health impact of interventions delivered by our services is 50% greater than if these same interventions were delivered by mainstream health services, primarily due to improved Indigenous access.5
All revenue is re-invested into our health services. There is no profit-taking. We reinvest in our Indigenous workforce and in locally-designed strategies to trial new approaches. We are part of Indigenous communities and understand how critical respectful community engagement is to improving health outcomes.
We have a high level of community oversight and accountability. Our boards are made up of local Indigenous people and we serve our communities. We are responsive to their needs and they are not shy to tell us to lift our game, if we disappoint. We have innovative, robust and flexible service models grounded in the culture of our people and contemporary primary health care practices.
7.Governments and communities have invested in the sector and have grown it over time — it is a valuable health asset
Our community controlled health services are an integral part of the Australian health system just as hospitals are. An exemption under section 19(2) of the Health Insurance Act 1973 allows Aboriginal controlled health services access to Commonwealth funding, even if they are funded by state governments.6 This flexibility allows all parties to work closely together to provide the full service offer and get the best outcomes according to local need and circumstances.
There are many examples of important partnerships between our services and mainstream providers working collaboratively to maximize impact. For example, in Western NSW, the roll-out of a new partnership saw the number of Aboriginal people using integrated care services for chronic conditions more than double in the space of just four months.7
The health system is increasingly complex in nature and the dire state of Indigenous health has meant that Aboriginal people need to have control over their own health response and be part of the solution. We work closely with mainstream services to extend the reach of services and share our expertise to improve cultural safety.
While governments struggle to deliver service models that rarely reach or effectively service the needs of the most vulnerable Aboriginal people, we excel. That’s because we are Aboriginal people who understand what is required to change the future health of our people and we deliver it.
6.Most of our staff are Indigenous, but we need more Indigenous clinical staff
Our network provides a critical and practical pathway into employment for many Indigenous people. Currently, 56% of our staff are Indigenous. The greater representation is amongst non-clinical staff.
Much more needs to be done to develop viable career pathways to get more Indigenous doctors, nurses and allied health professionals. Across Australia, there are only about 170 Indigenous medical practitioners, 730 allied health professionals, and 2,190 nurses.8
Source: Healthy Futures
9.We are the largest employer of Indigenous people
Our 141 Aboriginal controlled health services employ about 6,000 staff (most of whom are Indigenous). This means that one out of every 44 Indigenous jobs in Australia is with one of our services (3,300 of 141,400 FTE: 2.33%). This puts us well ahead of all mining employers. This is in a context where the health and social care sector employs 15% of the Aboriginal and Torres Strait Islander workforce; almost four times as many as the mining industry (4%).9
Our large network of services is also critical to the economic health of many remote and local communities.
10.The need is compelling
Good progress has been made, but Indigenous health is still vulnerable to disturbing developments such as the recent outbreak of congenital syphilis across regions of Northern Australia.
This is an entirely preventable disease not seen in Australia for generations and its occurrence raises concerns about the delivery of antenatal care and sexually transmitted infection and blood borne virus control programs for all high risk groups.
2.1 NSW : Sydney Close the Gap Picnic Breakfast event Surry Hills event
2.2 NSW : Awabakal ACCHO Close the Gap event : Expanding services to the Port Stephens community
To celebrate National Close The Gap day on Thursday 15th March, Awabakal is excited to announce that we are expanding our services to the Port Stephens community.
You are invited to the grand opening of our Raymond Terrace site!!
88 Port Stephens St Raymond Terrace
Thursday 15th March @ 11:30am.
This is our contribution to close the health and life expectancy gap between the Aboriginal and the non-Indigenous communities in our area.
We look forward to working with you and your family towards a healthier community.
2.3: NSW : Ready Mob and Galambila help Close the Gap at Bowraville Indigenous Health Workforce Expo. #FutureHealthChampions
The Ready Mob and Galambila ACCHO Coffs Harbour was pleased to participate in the Indigenous health workforce expo at the Bowraville Central School on Friday, 9 March. Pictured above with Karl Briscoe CEO NATSIHWA
This event was a first for a number of peak Aboriginal Health bodies and stakeholders that informed and inspired Indigenous students and their families in Bowraville and surrounding areas to pursue careers in health.
Alongside the Congress of Aboriginal and Torres Strait Islander Nurses and Midwives (CATSINaM), Indigenous Allied Health Australia (IAHA), the National Aboriginal and Torres Strait Islander Health Worker Association (NATSIHWA) and the Mid North Coast Local Health District (MNCLHD), AIDA had more than 30 Indigenous doctors, nurses, midwives, nutritionists, and physiotherapists attending the school to deliver activities demonstrating some of the day-to-day procedures that occur in their respective fields.
Through applying plaster casts, delivering a mannequin baby, operating on organs and participating in pre-game exercises undertaken by players from the St Kilda and Melbourne Victory teams, showed students the variety of jobs available to them if they embark on careers in health.
CATSINaM CEO Janine Mohamed says “building the Aboriginal and Torres Strait Islander health workforce through targeted investment in our young people is critical to closing the gap on health disadvantage – we are proud to be part of an initiative that works with our communities in delivering a tailored approach to health education and training pathways”.
NATSIHWA CEO Karl Briscoe is proud to participate in the event, which will showcase what is possible for the Aboriginal youth of Bowraville who wish to commence a career in the health sector. “There are many pathways for our youth and we are thrilled to help foster and support our next generation of Aboriginal Health Workers and Aboriginal Health Practitioners”.
IAHA Chairperson Nicole Turner says “we know that if we want to see long-term sustainable change to health outcomes, we need a strong representation of Aboriginal and Torres Strait Islander health practitioners and workers across the many diverse careers in health. Engaging our young people and sharing the amazing opportunities available is part of growing that health workforce into the future”.
AIDA President Dr Kali Hayward says “it is so encouraging that we have so many people, organisations, families and community members supporting this important event. We are really excited to bring Indigenous health workers into the community to engage with students about the many options they have regarding careers in health”.
The MNCLHD has been instrumental in pulling this event together at the local level and engaging with the community to ensure this event is a success for everyone who attends. It is inspiring to see this level of enthusiasm in the community.
3.1 NT : Danila Dilba ACCHO Close the Gap event Darwin
Today 15 March is Close The Gap day. From 9:30AM to 11AM Danila Dilba will be at Stuart Park Pharmacy, 4/5 Westralia St, Stuart Park.
There will be food and giveaways supplied by the pharmacy. Danila Dilba will have information stalls and Hearing Australia will be there as well doing free hearing checks.
Radio Larrakia will also be broadcasting live from the event. Come on down tomorrow for this important day.
3. 2 NT : Congress Alice Springs and CASSE Close the Gap _- Aboriginal Male Health
” Establishing a male leadership group, having a place for males and addressing violence have been identified as key priorities in a research project to investigate ways to develop a best practice Aboriginal Men’s Shed in Alice Springs.
The Kurruna Mwarre-Ingkintja (Good Spirit Males Place) Research Project, a collaboration between the Central Australian Aboriginal Congress (Congress) and Creating A Safe Supportive Environment (CASSE) – commenced in 2015 with the aim of developing a unique Aboriginal Men’s Shed Model, along cultural lines, to empower men to find their voices and live authentically.
For two years prior, many consultations were held with Aboriginal men and communities to determine the direction and need for pending research. The research has been philanthropically funded.”
The completed research report was launched at THE OLD COURTHOUSE, ALICE SPRINGS
Ken Lechleitner Pangarte, the primary Researcher Officer, is an Anmatjere and Western Arrernte man with a cultural reputation for being able to move between the two worlds and for being an advocate for change for his people.
On establishing a male leadership group, Ken said: “This group of males shaped the direction of where the research should go, not to the bookshelves to gather dust, but create an entity to ensure findings are implemented into becoming outcomes.”
The group identified the need for new Aboriginal organisations, while operating alongside, and to provide a place for men to go to receive the physical, social and psychological support they need to get their lives on track, leading to establishment of the Blokes On Track Aboriginal Corporation (BOTAC).
“Establishing BOTAC was a breakthrough in finding a solution to engaging multiple services and these services have indicated that they would be happy working with a mutual body like BOTAC providing the required male leadership,” Ken stated.
The project included qualitative research interviews with 23 male participants living in Alice Springs that illuminated critical aspects of men’s experiences. Fourteen of the men agreed to have their interviews on public record and are published in “Talking Powerfully from the Heart – Interviews by Ken Lechleitner”, providing a moving adjunct to the research report.
“Their interviews brought to light and to life new found voices for males from central Australia,” Ken said.
Pamela Nathan, Director of CASSE’s Aboriginal Australian Relations Program, Senior Investigator, co-supervised the project and stated that the interviews “illuminated critical aspects of men’s experiences. Their recognition of the degree to which they have unmet emotional and psychological needs was striking – an aspect of their experience that seemed unrecognised by the wider public.
“The men say they hide their feelings that ‘they hurt, they bleed they have pain’, ‘all suffering’, feel ‘degraded and scorned’, ‘disempowered’, ‘lost’, ‘devalued’ and ‘unrecognised,’ seen as ‘violent losers’ and more.”
A key component of the project was trialling the psychoanalytically informed 15week ‘BreakThrough Violence’ group treatment program for the prevention and treatment of violence. The program privileges cultural and emotional experiences.
The summary of participants in the group program is an indictment of the system –many of the men were repeat violent offenders and many had not before received treatment for violence, let alone treatment in a culturally appropriate manner:
32 men regularly participated in the weekly program
over two thirds (23 men) had not attended a violence treatment program before
nearly all (30) of the men were mandated
over two-thirds (20 men) had committed violent offences
21 of the men had been in gaol before
15 had been in gaol at least twice if not more often.
5 of the men had been in gaol over five times.
23 of the men were substance affected at the time of the offence.
The majority of men were aged between 20 and 40
Half the men lived in remote communities, with slightly less living in town
30 out of the 34 men said they found the group helpful.
Final recommendations from the Kurruna Mwarre-Ingkintja Research Project report include:
Establish a services agreement between Non-Government and Government Organisations through Blokes On Track Aboriginal Corporation (BOTAC)
Establishment of Male Cultural Place
Establishment of Psychological Place Health Retreat
Men’s Residential area
Chronic Disease Care Management services to be provided into the Male place
Palliative Care Services on Country
Establish a lease agreement with Iwupataka Land Trust
7.1 Public Space area
7.2 Restaurant / Café
7.3 Market Place
For over 40 years, Central Australian Aboriginal Congress (Congress) has provided support and advocacy for Aboriginal people in the struggle for justice and equity. Since that time, Congress has expanded to become the largest Aboriginal community-controlled health organisation in the Northern Territory, providing a comprehensive, holistic and culturally-appropriate primary health care service to Aboriginal people living in and nearby Alice Springs, including five remote communities; Amoonguna, Ntaria (and Wallace Rockhole), Santa Teresa, Utju (Areyonga) and Mutitjulu. Today, we are one of the most experienced Aboriginal primary health care services in the country, a strong political advocate of closing the gap on Aboriginal health disadvantage and a national leader in improving health outcomes for all Aboriginal people.
CASSE (Creating A Safe Supportive environment) is a psychological not-for-profit organisation with the vision to change minds in order to save lives. CASSE aims to promote safe, supportive environments through psychoanalytic awareness. We focus on empowering people and communities to understand and work through their trauma (manifest by suicide, depression, violence, substance usage) by preserving and strengthening cultural life and capacity between the generations in a self-determining way.
4.WA AHCWA is hosting a Close the Gap Family Festival!
There will be live entertainment, traditional dancers, 100.9fm Noongar Radio, community stalls, food vans, animal farm, face painting, traditional art, seniors tent, photo booth, raffles and heaps more!
Key details: 24th March, 2018 at Birdwood Park, Highgate, from 11am-5pm!
Please share through your networks and make sure you come down
5. ACT : Winnunga ACCHO helping to Close the Gap in the ACT
The Ngunnawal people are the Traditional Owners of the lands that the ACT is located on. However, there are many Aboriginal people from other parts of the country living in and visiting Canberra. This is mainly due to the mobility of people generally, connecting with family, the histories of displacement, and employment opportunities particularly in the Commonwealth public service.
Winnunga was established in 1988 by local Aboriginal people inspired by the national mobilisation of people around the opening of the new Parliament House in May and the visit by the Queen. The late Olive Brown, a particularly inspirational figure who worked tirelessly for the health of Aboriginal people, saw the need to set up a temporary medical service at the Tent Embassy site in Canberra and this proved to be the beginning of Winnunga.
Mrs Brown enlisted the support of Dr Sally Creasey, Carolyn Patterson (registered nurse/midwife), Margaret McCleod and others to assist. Soon after ACT Health offered Mrs Brown a room in the office behind the Griffin Centre to run a clinic twice a week (Tuesday and Thursday mornings) and on Saturday mornings.
Winnunga operated out of this office from 1988 to 1990. The then Winnunga Medical Director, Dr Peter Sharp, began work at Winnunga in 1989. Other staff worked as volunteers. In January 1990 the t ACT Minister for Health at the time, Wayne Berry, provided a small amount of funding. By 1991 the clinic was operating out of the Griffin Centre as a full time medical practice. In that same year the ACT attained self-government.
6.1 : QLD ATSICHS Brisbane team helps to Close the Gap at the women’s fun run
6.2 QLD : Telehealth closes the gap on Indigenous health in Queensland
“By having a telehealth-supported dementia service based at a primary health care centre, it means people will not have to travel to access care, and the videoconferencing equipment will be available for other services as well”
Cunnamulla Aboriginal Corporation for Health CEO Kerry Crumblin said areas previously not covered by specialist services would benefit from the program, and patients at high risk could be targeted
Centre Director Professor Anthony Smith said the service would provide specialist geriatric consultations via videoconference for people with dementia and their carers living in rural and remote areas of Queensland.
“Aboriginal and Torres Strait Islander people as young as 45 are being diagnosed with dementia, and Indigenous people experience the disease at a rate three to five times higher than the general population,” Professor Smith said.
The service, based at Brisbane’s Princess Alexandra Hospital and Cairns Hospital, aims to provide earlier diagnosis and better treatment.
The DREAMT project is funded by the Department of Health, Dementia and Aged Care Services Fund
7. Vic :VAHS is holding an event /Health checks for Closing the Gap Day.
CTG will be held at both Fitzroy and Preston sites.
During the day, there are going to be health information stalls and lunch. For people who haven’t had their health checks, and would like to book in for another time, today is your day!
As apart of having you health check completed, you can either receive a t-shirt or $30 voucher. Hope to see you there. Thank you
” Indigenous Affairs Minister Nigel Scullion ignored a plea from a government MP more than a year ago to implement a $25 million policy to combat sexually transmitted diseases gripping Aboriginal communities, instead adopting a $9m program that remains stalled.
The Australian has obtained a letter penned by Liberal senator Dean Smith warning that the rise of STIs in indigenous communities was “disturbing” and urged Senator Scullion to take immediate action, describing the situation as “critical”.
See Minister Scullion’s Correction part 2 below
” The Minister for Indigenous Health, Ken Wyatt, has confirmed that the surge response is not “stalled” as The Australian has claimed and is being rolled out in partnership with the States and Territories as well as Aboriginal Community Controlled Health Organisations.”
Front Page of the Australian this morning
“I’m sure you would agree that the increase in rates are disturbing and it’s critical that we tackle this challenge head on to ensure the problems do not escalate to a crisis point,” Senator Smith told Senator Scullion in December 2016.
When contacted yesterday about the letter, Senator Scullion shifted blame for the government’s inaction to Indigenous Health Minister Ken Wyatt.
Senator Scullion’s spokesman told The Australian he passed Senator Smith’s letter on to the “health portfolio”.
The letter, addressed to Senator Scullion and copied to Mr Wyatt and former health minister Sussan Ley, outlined a detailed proposal drafted by experts James Ward and Frank Bowden, in consultation with the National Aboriginal Community Controlled Health Organisation, to tackle a syphilis epidemic in indigenous communities.
Professor Ward yesterday confirmed he had meetings with Senator Scullion, Mr Wyatt and Health Minister Greg Hunt about his policy proposal. The Ward-Bowden policy was drafted following meetings with Ms Ley.
Six children have died from gestational syphilis since the epidemic emerged in north Queensland in 2011 and later spread to the Northern Territory, Western Australia and South Australia.
The government sat on the $25m policy until last November when it agreed to adopt one third of it as part of an $8.8m plan to tackle the syphilis outbreak in central and northern Australia.
The two other elements of the proposed three-year program — to reduce HIV risks and broader STI risks in Aboriginal communities — were rejected.
Since announcing the watered-down policy, the government has failed to rollout the program despite bureaucrats holding meetings about its implementation since August, before its funding was signed off by Mr Wyatt.
Mr Wyatt said yesterday the rollout would begin in Cairns and Darwin in May. He said the syphilis outbreak was an “absolute priority” and had been targeted on a national basis since 2015 but more funding was needed because the states had not contained it.
“This is why the Chief Medical Officer is leading a nationally co-ordinated enhanced response to the outbreak in conjunction with states and territories who have the primary role for delivering sexual health services and dealing with infectious disease outbreaks,” Mr Wyatt said.
Professor Ward said adopting only a third of the policy would reduce its efficacy and cost the community more money to address the problem in the long term.
“We put it to them in December 2016 and they still haven’t rolled out any of it. I don’t mean to make any judgment about whether they are dragging their heels or not,” Professor Ward said.
Olga Havnen, chief executive of the Darwin-based Danila Dilba health service, said she was consulted on Professor Ward’s policy and expressed anger it had not been adopted in full.
“It is obscene, it is ridiculous. If you are going to tackle STIs then it would have made sense to do a comprehensive response,” she said. “This is a preventable disease and, I can tell you now, if this was happening in the major suburbs of Sydney or Melbourne there would have been urgent and immediate action.”
Retired Aboriginal magistrate Sue Gordon, who chaired the Howard government’s Northern Territory intervention taskforce, said it was about time state and federal governments took the issue seriously.
Labor indigenous senator Pat Dodson said: “The government has not taken the outbreak seriously enough and have not taken appropriate action to tackle the outbreak, otherwise we would not be in this situation.”
Part 2 **CORRECTION**
Minister for Indigenous Affairs Senator the Hon. Nigel Scullion
Correction to incorrect reporting in The Australian newspaper
Thursday 15 March 2018
Today’s Australian article by Greg Brown, Sex disease warning ignored, incorrectly states I ignored a letter by Senator Dean Smith in December 2016 regarding a plan to tackle increasing rates of Sexually Transmissible Infections (STIs) in the Indigenous population.
This is grossly misleading and entirely incorrect. I did not ignore Senator Smith’s letter or the request contained in it but referred it to the Indigenous Health portfolio as the relevant and appropriate portfolio with responsibility for Indigenous Health issues. I responded to Senator Smith on this basis.
Notwithstanding that States and Territories have primary responsibility for delivering sexual health services and dealing with infectious disease outbreaks, the Minister for Indigenous Health announced a nationally coordinated surge response in November last year to address the rising rates of STIs in the Aboriginal and Torres Strait Islander population.
The Minister for Indigenous Health, Ken Wyatt, has confirmed that the surge response is not “stalled” as The Australian has claimed and is being rolled out in partnership with the States and Territories as well as Aboriginal Community Controlled Health Organisations.
Questions about the status of the surge response or the proposal referred to in this article should be referred to the Department of Health, as is appropriate.
To suggest however that I ignored any warnings regarding the protection of human life is absolutely repugnant and appalling and I reject any such assertion unequivocally.
This is yet another example of ill-informed and incorrect reporting of Indigenous issues by The Australian newspaper.