
” National media outlets ( Including Peta Credlin on SkyNews and News Corp Newspapers see Part 5 below plus Today Tonight SA ) have aired wrongful claims that the codes would force white nurses to ‘apologise to Indigenous clients for being white’.
The codes do not say that – that idea was invented and then pushed on these media programs.
These stories were not based in facts, but seem to have been driven by the partisan politics of a fringe nursing group, and conservative politicians who have been approached to comment on the wrongful claims.
I am sure that some of our nursing and midwifery members and community will be hearing disturbing claims.
Let me be clear, nurses and midwives under the new code do not have to announce their ‘white privilege’ before treating Indigenous clients.
I am really proud of these new codes, and not only because the Congress of Aboriginal and Torres Strait Islander Nurses and Midwives (CATSINaM) contributed to their development, which included extensive consultation across nursing and midwifery and at the time no one opposed the inclusion of cultural safety “
Janine Mohamed CEO CATSINaM see IndigenousX Part 1 below
Read over 90 NACCHO Aboriginal Health and Racism articles published last 6 Years
Read 30 NACCHO Aboriginal Health and Cultural Safety published last 6 years
” It is clear from the 2018 Closing the Gap Report tabled by Prime Minister Turnbull in February 2018 that Aboriginal and/or Torres Strait Islander Peoples still experience poorer health outcomes than non-Indigenous Australians.
It is well understood these inequities are a result of the colonisation process and the many discriminatory policies to which Aboriginal and/or Torres Strait Islander Australians were subjected to, and the ongoing experience of discrimination today.
All healthcare leaders and health professionals have a role to play in closing the gap.
The approach the NMBA has taken for nurses and midwives (the largest workforce in the healthcare system) by setting expectations around culturally safe practice, reflects the current expectations of governments to provide a culturally safe health system.
(For more information please see the COAG Health Council 4 August 2017 Communiqué).
Combined Press Release Nursing and Midwifery Board of Australia ,The Australian Nursing and Midwifery Federation, the Australian College of Nursing, the Australian College of Midwives and the Congress of Aboriginal and Torres Strait see in full Part 2 Below
” I was stunned to read businessman Graeme Haycroft’s comments regarding nurses and indigenous Australians on the weekend, as part of his criticism of the new NMBA Codes and the term cultural safety which is defined in a glossary connected to the codes.
These codes were the subject of lengthy consultations with the professions of nursing and midwifery and other stakeholders including community representatives.
This review was comprehensive and evidenced-based. Our union and our national body the Australian Nursing Midwifery Federation (ANMF) were active participants in these consultations.
The codes, written by nurses and midwives for nurses and midwives, seek to ensure the individual needs and backgrounds of each patient are taken into account during treatment.”
QNMU Secretary Beth Mohle issued a statement clarifying misleading comments in the media around the NMBA’s new Codes of Conduct for nurses and midwives: See in Full part 3 Below
” And just to reinforce that point, the entire premise for the segment was false.
There is no requirement for nurses to apologise for being white, which would be very awkward for the more the more than 1500 Indigenous nurses across Australia, and the countless others who also aren’t white to begin with. But, even for the nurses who are – THERE IS NO REQUIREMENT FOR THEM TO APOLOGISE FOR BEING WHITE.
So, why on Earth would Today Tonight run such a story?
Why would they base a story off the demonstrably false allegations of this Graeme Haycroft person? “
The truth behind the Nursing Code of Conduct lie ; Indigenous X Article Read in full Part 4
Catch Up: Having to apologise for being white – the controversial new code for nurses treating Indigenous Australians. #TTAdelaide pic.twitter.com/yViiqkw67F
— TodayTonightAdelaide (@TodayTonightSA) March 23, 2018
If you thought nursing was about quality health care, think again.
According to the Nursing and Midwifery Board of Australia, “’cultural safety’ is as important to quality care as clinical safety”. And there’s no objective test of ‘cultural safety’; it’s determined, so the Board says, by the “recipient of care”. You see, it’s not just what the nurse does that matters but “how a health professional does something”.”
Graeme Haycroft from @NursesPAQ: There's 350,000 nurses and midwives Australia-wide and they're all subject to this code which encourages them to recognise their 'white privilege'.
MORE: https://t.co/iphNgaZ53F #Credlin pic.twitter.com/ThzGSocmob
— Sky News Australia (@SkyNewsAust) March 21, 2018
So who is this Graeme Haycroft

Businessman . Director of Queensland Association Services Group (QAS Group), Political activist , Anti Unionist
And according to peak Nurses groups Graeme has has no previous health experience or qualifications
Graeme has spent a lifetime working in industrial relations and was the man who set up Haycroft Workplace Solutions, leading provider of workplace consulting and management that has nearly 2000 workers on the payroll.
He is chair of the Liberal National Party’s labour market policy committee, active in the HR Nicholls Society, is a regular commentator on labour market issues, and has published his thoughts in such places as the IPA Review, Courier Mail and Online Opinion. But Graeme’s most important contributions have come through what he has done, not what he has written or said.
In the 1990s Graeme famously fought the Australian Workers’ Union to set up sub-contracting for shearers in Charleville, and went on to battle the CMFEU in helping to set up union-free high-rise construction sites. When the Howard government allowed Australian Workplace Agreements (AWAs), Graeme was instrumental in creating the most widely copied template in the country, and his business helped set up about 30,000 agreements.
Lately, Graeme has been working on a exciting new project with the potential to fundamentally change the role and power of unions in this country, while improving services for workers.
He is not waiting for politicians to act; he is changing the system himself… and after years of planning he is finally ready to show us how.
So who is this new Nurses Professional Association of Queensland ?
Queensland Association Services Group QAS Group and Sajen Legal have established a new business model for Employee Associations Queensland Association Services Group (QAS Group), who are the contracted service providers for the NPAQ, in conjunction with Sajen Legal have developed and set up a new association business model.
Working with a small group of dedicated and experienced nurses, they have built in a strict separation between the money earned and spent on the one hand, and the control of the Association on the other.
To launch NPAQ, the QAS Group , have backed the provision of services for ten years under contract. They have provided all of the seed funding for the administrative and legal services including the member Professional Indemnity Insurance policy required of the Association..
Whilst it will be many years before all the seed funding is fully repaid, at the end of our second year, the membership income was sufficient to fund all the running expenses of the NPAQ
” And they quote no party politics “
The NPAQ executive is resolute that there will be no party politics. Every cent of your NPAQ membership money is spent on nurse services and issues
When NACCHO pointed out that NursesPAQ was ” using the definitions of two America right wing commentators to justify mounting a political membership campaign in which you sensationalise and falsely quote out of context aspects of our Indigenous cultural safety in Australia ”
These videos were then removed from the NPAQ news page
http://www.npaq.com.au/news.php
Part 1 Janine Mohamed CEO CATSINaM

Originally Published Indigenous X
I rang my dad over the weekend. We’d hardly begun yarning before he asked me: “What’s this about white nurses having to apologise to us for being white?”
I could have just said, “Dad, you should know better than to believe what the mainstream media says about us.”
But instead I took the time to explain the truth behind recent misleading media reports on new codes of conduct for nurses and midwives.
Media outlets have aired wrongful claims that the codes would force white nurses to ‘apologise to Indigenous clients for being white’.
The codes do not say that – that idea was invented and then pushed on these media programs.
As Luke Pearson recently wrote for IndigenousX, these stories were not based in facts, but seem to have been driven by the partisan politics of a fringe nursing group, and conservative politicians who have been approached to comment on the wrongful claims.
I took the time to have the conversation with my Dad because it is important people understand how significant these new codes are for efforts to improve the care of our people, hence I thought it important to reach out to the readers of IndigenousX too.
I am sure that some of our nursing and midwifery members and community will be hearing disturbing claims.
Let me be clear, nurses and midwives under the new code do not have to announce their ‘white privilege’ before treating Indigenous clients.
I also had the conversation because, to be honest, I am really proud of these new codes, and not only because the Congress of Aboriginal and Torres Strait Islander Nurses and Midwives (CATSINaM) contributed to their development, which included extensive consultation across nursing and midwifery and at the time no one opposed the inclusion of cultural safety.
We are delighted the Nursing and Midwifery Board of Australia (NMBA) listened to CATSINaM in developing these new codes, and took on board our advice that cultural safety should be recognised as an integral part of ethical and competent professional practice. Further, they cited some of our work at CATSINaM in materials supporting the code.
CATSINaM has been at the forefront of advocating for cultural safety training for health professionals at all levels of health systems in order to improve care for both Indigenous clients and their families. Improving the cultural safety of workplaces is also a vital strategy for improving the recruitment and retention of Indigenous health professionals and staff. We need more of our people in the health system.
Rather than being criticised by sensationalist, inaccurate reports, the NMBA deserves credit for showing leadership in the area of cultural safety. They have set a great example for other health professions and organisations. It wouldn’t be the first time that nurses and midwives have been at the forefront of leading change.
In fact, this is also not the first time this has happened. In many ways, Australia is playing a game of ‘catch up’.
In New Zealand, cultural safety is part of the nursing and midwifery code of conduct and also in the laws that nurses and midwives must follow to be registered to practice. This happened well over 10 years ago because many Maori nurses worked hard for many years to teach their non-Maori colleagues about cultural safety and gain their support so they could provide better care for their people. This is considered completely normal in New Zealand.
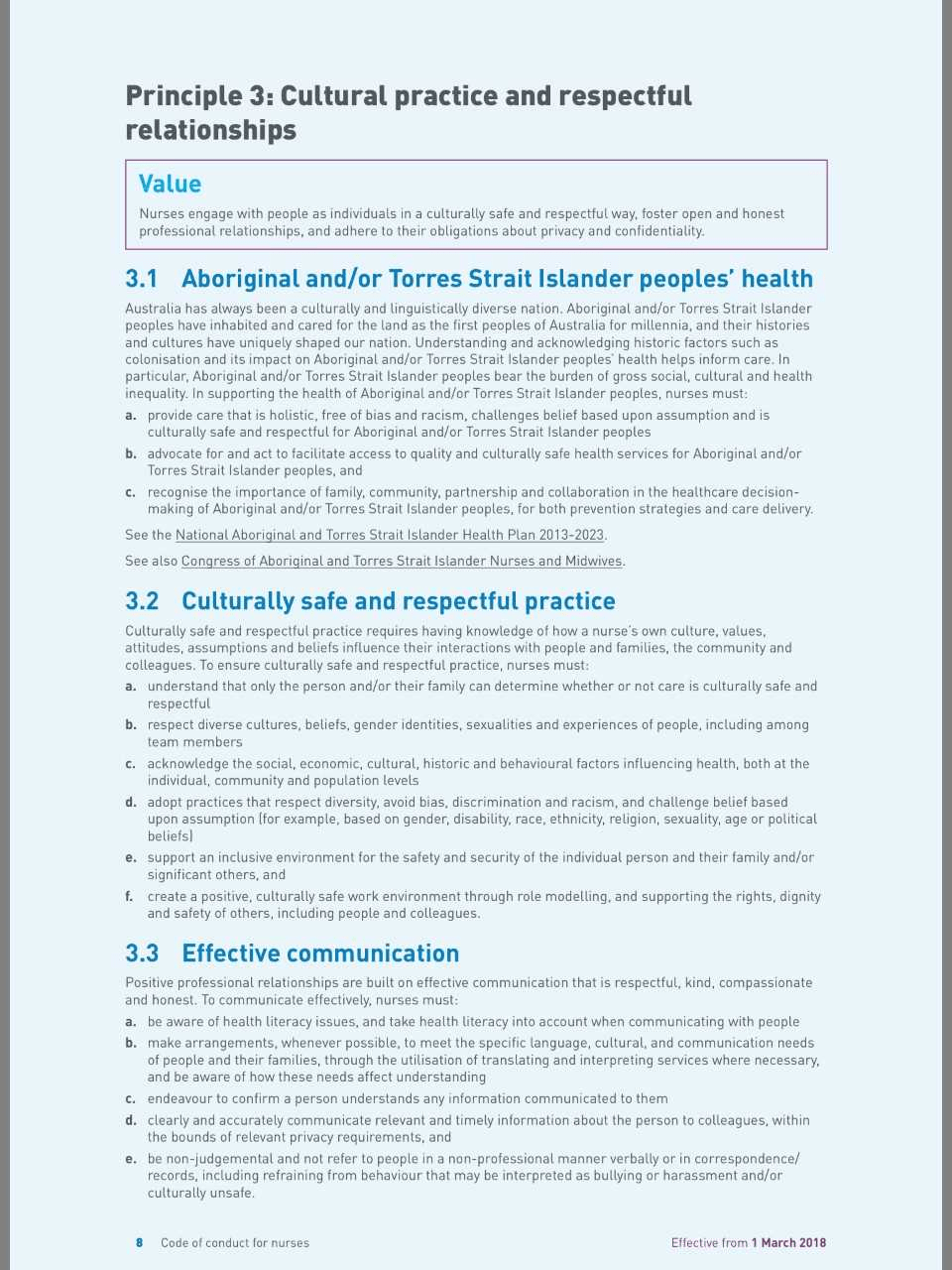
Under the new codes, which took effect on 1 March, nurses and midwives must take responsibility for improving the cultural safety of health services and systems for Aboriginal and Torres Strait Islander clients and colleagues.
They are required to provide care that is “holistic, free of bias and racism”, and to recognise the importance of family, community, partnership and collaboration in the healthcare decision-making of Aboriginal and/or Torres Strait Islander people.
The codes advocate for culturally safe and respectful practice and require nurses to understand how their own culture, values, attitudes, assumptions and beliefs influence their interactions with people and families, the community and colleagues (for more information on our position on Cultural Safety please visit our website).
As part of such reflexive practice, nurses and midwives are encouraged to consider issues, such as white privilege, and how this can affect the assumptions and practices they bring to the care of clients and how they interact with their families. It must be said that privilege has been discussed in Australia for some time – although we are more used to talk about class privilege in Australia – those who have more financial resources compared to those who don’t.
Over time we have recognised there different forms of privilege – men have male privilege in contrast to women. Able-bodied people have able-bodied privilege compared to people living with different types of disabilities. Heterosexual people have heterosexual privilege compared to people who are lesbian, gay, bisexual, transgender, intersex or queer. Not to mention what we have been socialised to believe is normal!
Many people have campaigned for decades to help us learn about these different forms of privilege and do something to change inequity they cause. This has involved education, advocacy, legislation, policies and professional codes of conduct. The acknowledgement of these different forms of privilege and the non-acceptance of biased treatment has resulted in improved circumstances for women, people living with disabilities and lesbian, gay, bisexual, transgender, intersex or queer people. But there is still a long way to go in all of these areas, and especially so where they intersect.
There has been considerable work over the last 20-30 years to talk about white privilege and address the inequity that many white Australians don’t see or realise is there, although Aboriginal and Torres Strait Islander Australians live this every day.
Cultural safety training does include examining how Indigenous people have been locked out of the opportunities that most white people take for granted by past policies and this has resulted in intergenerational exclusion and Indigenous disadvantage. This means that white privilege is one of the areas that people must explore and understand. This is what the codes are asking nurses and midwives to do – to think this through so they do not make incorrect and unhelpful assumptions based on their idea of what is normal for non-Indigenous Australians, particularly white Australians.
A glossary accompanying the new codes cites CATSINaM materials. It identifies that the concept of cultural safety was developed more than 20 years ago in a First Nations’ context (in New Zealand) and holds that the recipient of care – rather than the caregiver – determines whether care is culturally safe. That means you determine if the care you receive is culturally safe.
Instead of providing care regardless of difference, such as when people say ‘I treat everyone the same’, to providing care that takes account of peoples’ unique needs. This includes their cultural needs.
While this is important for Indigenous clients, it also has the potential to improve all clients’ care by encouraging health practitioners to be more reflexive and responsive to the needs of different clients.
Despite what recent headlines might have us believe, there is widespread support for cultural safety’s implementation across the health system.
The National Aboriginal and Torres Strait Islander Health Plan: 2013-2023 (2015) and its associated Implementation Plan (both available here) identify the importance of cultural safety in addressing racism in the health system, and many health services already provide cultural safety training for their staff.
The Australian Nursing and Midwifery Federation, the Australian College of Nursing, the Australian College of Midwives are united with CATSINaM in strongly supporting the guidance around cultural safety in the new codes of conduct.
The Council of Deans of Nursing and Midwifery also considers cultural safety an integral part of competencies for registered nurses and midwives. Providing culturally safe care that is free from racism should be a normal expectation. All health professionals learning about cultural safety and building it into their codes of conduct is a very important step to this becoming a reality. Hence nurses and midwives are currently required to study Aboriginal and Torres Strait Islander health, culture, history, and cultural safety as part of their study programs.
Cultural safety is talked about and implemented in other fields, including education, and family and community services, although people in these fields are still learning about it so it is not always standard practice yet. In fact, CATSINaM recommended cultural safety training for journalists in our submission to the recent Senate Inquiry into the future of public interest journalism, and the latest media fracas indicates just how sorely this is needed.
It is important that we continue these conversations about the importance of cultural safety for healthcare and other systems – they are potentially life-saving.

For readers who wish to contribute to the discussion, I suggest you read the joint statement from nursing and midwifery organisations and the codes of conduct, which can be downloaded here.
Part 2

In response to Graeme Haycroft’s recent comments, we welcome the opportunity to provide further information on how important cultural safety is for improving health outcomes and experiences for Aboriginal and Torres Strait Islander Peoples.
It is clear from the 2018 Closing the Gap Report tabled by Prime Minister Turnbull in February 2018 that Aboriginal and/or Torres Strait Islander Peoples still experience poorer health outcomes than non-Indigenous Australians. It is well understood these inequities are a result of the colonisation process and the many discriminatory policies to which Aboriginal and/or Torres Strait Islander Australians were subjected to, and the ongoing experience of discrimination today.
All healthcare leaders and health professionals have a role to play in closing the gap.
The approach the NMBA has taken for nurses and midwives (the largest workforce in the healthcare system) by setting expectations around culturally safe practice, reflects the current expectations of governments to provide a culturally safe health system. (For more information please see the COAG Health Council 4 August 2017 Communiqué).
Culturally safe and respectful practice is not a new concept. Nurses and midwives are expected to engage with all people as individuals in a culturally safe and respectful way, foster open, honest and compassionate professional relationships, and adhere to their obligations about privacy and confidentiality.
Many health services already provide cultural safety training for their staff. Cultural safety is about the person who is providing care reflecting on their own assumptions and culture in order to work in a genuine partnership with Aboriginal and Torres Strait Islander Peoples.
Nurses and midwives have always had a responsibility to provide care that contributes to the best possible outcome for the person/woman they are caring for. They need to work in partnership with that person/woman to do so. The principle of cultural safety in the new Code of conduct for nurses and Code of conduct for midwives (the codes) provides simple, common sense guidance on how to work in a partnership with Aboriginal and Torres Strait Islander Peoples. The codes do not require nurses or midwives to declare or apologise for white privilege.
The guidance around cultural safety in the codes sets out clearly the behaviours that are expected of nurses and midwives, and the standard of conduct that patients and their families can expect. It is vital guidance for improving health outcomes and experiences for Aboriginal and Torres Strait Islander Peoples.
The codes were developed through an evidence-based and extensive consultation process conducted over a two-year period. Their development included literature reviews to ensure they were based on the best available international and Australian evidence, as well as an analysis of complaints about the conduct of nurses and midwives to ensure they were meeting the public’s needs.
The consultation and input from the public and professions included working groups, focus groups and preliminary and public consultation. The public consultation phase included a campaign to encourage nurses and midwives to provide feedback.
The Australian Nursing and Midwifery Federation, the Australian College of Nursing, the Australian College of Midwives and the Congress of Aboriginal and Torres Strait Islander Nurses and Midwives all participated in each stage of the development and consultation of the new codes. The organisations strongly support the guidance around cultural safety in the codes for nurses and midwives.
| Lynette Cusack
Chair Nursing and Midwifery Board of Australia |
Ann Kinnear
CEO |
Kylie Ward
CEO |
Janine Mohamed
CEO |
Annie Butler
A/Federal Secretary Australian Nursing and Midwifery |
For more information:
Part 3 QNMU Secretary Beth Mohle has issued a statement clarifying misleading comments in the media over the weekend around the NMBA’s new Codes of Conduct for nurses and midwives.

I was stunned to read businessman Graeme Haycroft’s comments regarding nurses and indigenous Australians on the weekend, as part of his criticism of the new NMBA Codes and the term cultural safety which is defined in a glossary connected to the codes.
These codes were the subject of lengthy consultations with the professions of nursing and midwifery and other stakeholders including community representatives. This review was comprehensive and evidenced-based. Our union and our national body the Australian Nursing Midwifery Federation (ANMF) were active participants in these consultations.
The codes, written by nurses and midwives for nurses and midwives, seek to ensure the individual needs and backgrounds of each patient are taken into account during treatment.
There’s no doubt cultural factors, including how a patient feels while within the health system, can impact wellbeing. For example, culture and background often determine how a patient would prefer to give birth or pass away.
Every day, nurses and midwives consider a range of complex factors, including a patient’s background and culture to determine the best treatment. These codes simply articulate what is required to support safe nursing and midwifery practice for all.
Mr Haycroft stated that the new code “has been sponsored and supported by the QNU to promote its party political social policy.”
This statement is disturbing on a number of levels. The Queensland Nurses and Midwives’ Union (QNMU) has repeatedly refuted Mr Haycroft’s allegations we donate to political parties. We do not. Nor are we affiliated with any political party. Yet Mr Haycroft continues to repeat these claims.
Secondly, this statement demonstrates a failure to understand the basics. It is the Nursing and Midwifery Board of Australia (NMBA) that regulates the practice of nurses and midwives through its standards, codes and guidelines.
The QNMU actively participates in NMBA consultations and represents the interests of our members individually and collectively. However, the new codes have not been “sponsored” by our union.
As a not-for-profit organisation run by nurses and midwives for nurses and midwives, the QNMU will remain steadfastly focused on advancing the values and interests of our members and the safety of those in their care. We will not be diverted by the political or business agendas of others.
Author Luke Pearson Indigenous X
But first tonight, the contentious new code telling nurses to say “sorry for being white” when treating their Indigenous patients.
That’s how Today Tonight Adelaide began last night.
It continued:
“Now, it’s the latest in a string of politically correct changes for the health industry, but this one has led to calls for the Nursing Board boss to resign.”
It was followed by a five minute story with the new code being condemned by someone you’ve probably never heard of, Graeme Haycroft, explaining that:
“According to how the code is written, the white nurse would come in and say, ‘before I deal with you, I have to acknowledge to you that I have certain privileges that you don’t have” followed by Cory Bernardi calling it divisive.
It goes on in this vein for a full five minutes before it cuts back to the presenter, who finally says, “The Nursing and Midwifery Board has told us that the code was drafted in consultation with Aboriginal groups and has been taken out of context as it’s not a requirement for health workers to declare or apologise for white privilege”.
And just to reinforce that point, the entire premise for the segment was false. There is no requirement for nurses to apologise for being white, which would be very awkward for the more the more than 1500 Indigenous nurses across Australia, and the countless others who also aren’t white to begin with. But, even for the nurses who are – THERE IS NO REQUIREMENT FOR THEM TO APOLOGISE FOR BEING WHITE.
So, why on Earth would Today Tonight run such a story?
Why would they base a story off the demonstrably false allegations of this Graeme Haycroft person?
To answer that, it might useful to cut back to a 2005 Sydney Morning Herald story about Mr Haycroft:
“A member of the National Party and the H.R. Nicholls Society, he (Mr Haycroft) boasts that, because of a tussle he had with the Australian Workers Union 15 years ago, the union does not have a single member shearing sheep in south-western Queensland today.
Now he runs a labour hire firm with a thriving sideline in moving small-business employees off awards and collective agreements and onto the Federal Government’s preferred individual contracts, Australian Workplace Agreements.
…Mr Haycroft’s business stands out because he is targeting lower-skilled, lower-paid workers, often with poor English – the people unions say have much to fear from individual contracts.”
Cut back to 2018, and Graeme Haycroft now runs the Nurses Professional Association of Queensland, which promotes itself as an alternative to the Qld Nurses Union.
So, a man with a long history of fighting Unions, who ‘saved’ the mushroom farming business by showing businesses how to move “small-business employees off awards and collective agreements and onto the Federal Government’s preferred individual contracts, Australian Workplace Agreements.”
According to the 2005 article, “Mr Haycroft said workers had been more than happy to sign on, most with their penalty rates, holiday pay and other conditions being rolled into a flat rate.”
“However, [there is always a ‘however’], Mr Haycroft was stripped of his preferred provider status with the Office of the Employment Advocate on Thursday, after a Sydney picker, Carmen Walacz Vel Walewska, said she was sacked after she contacted the Australian Workers Union for advice on AWAs.”
With that track record, it’s hard to imagine why nurses would want to leave their current union in favour of his ‘professional association’.
It seems as though, once again, Indigenous people have become a political football and a convenient scapegoat for issues that have nothing to do with us.
Queensland has a long history of political success found through anti-Aboriginal sentiment, so what better way to undermine a Union and recruit new members to a professional association than to accuse the Union of ‘racism against white people’ and ‘political correctness gone made’ by spreading the blatantly false and misleading accusation that white nurses now have to apologise to Aboriginal people for being white?
And just like Dick Smith’s anti-immigration campaign, Blair Cottrell’s anti-African ‘community safety group’, and Prue McSween’s call for a new Stolen Generation, it seems Channel 7 is always more than happy to ignore the facts and sensationalise issues about race and racism.
There is always one more thing.
We, and others, will soon publish articles explaining what the Code of Conduct actually calls for, and explain why cultural competence and cultural safety are important (editor’s note: we did, here’s one of them), but I can’t help but be reminded of this quote from Toni Morrison:
“The function, the very serious function of racism is distraction. It keeps you from doing your work. It keeps you explaining, over and over again, your reason for being. Somebody says you have no language and you spend twenty years proving that you do. Somebody says your head isn’t shaped properly so you have scientists working on the fact that it is. Somebody says you have no art, so you dredge that up. Somebody says you have no kingdoms, so you dredge that up. None of this is necessary. There will always be one more thing.”
So, instead of working on the very real business of ensuring best practice within the nursing industry, our Indigenous experts in this area will have to take a few days away from this important work to explain that no one is asking for white nurses to apologise for being white.
Just like we have to explain that not all Aboriginal parents abuse their children, or that we don’t want to steal white people’s backyards, or that we had (and have) science, or that Australia wasn’t Terra Nullius, or, as Malcolm Turnbull suggested last year, that acknowledging Indigenous history and addressing the issue of colonial statues and place names across Australia is not a “Stalinist exercise of trying to wipe out or obliterate or blank out parts of our history”.
So long as Australian media and politics finds value, profit and opportunity in promoting racism, there will always be one more thing.
So, I might as well clear up a few others while I’m here, and empty a few more buckets out of the endless ocean of racist misinformation.
Child abuse isn’t a ‘cultural’ thing.
Police are not scared to arrest Aboriginal people out of fear of being called racist.
We don’t get free houses.
Aboriginal people using white ochre on their faces in dance and ceremony is not the same thing as white people dressing up in blackface.
We don’t get free university.
The Voice to Parliament is not a third chamber of parliament.
We are not the problem.
Anything else?
We aren’t vampires?
We don’t shoot laser beams out of our eyes?
We aren’t secretly developing a perpetual motion machine that runs on white tears?
I’m sure I, and countless others, will undoubtedly need to keep adding to this list because, as Toni Morrison tells us, there will always be one more thing.

If you thought nursing was about quality health care, think again.
According to the Nursing and Midwifery Board of Australia, “’cultural safety’ is as important to quality care as clinical safety”. And there’s no objective test of ‘cultural safety’; it’s determined, so the Board says, by the “recipient of care”. You see, it’s not just what the nurse does that matters but “how a health professional does something”.
According to the commissars at the Board, “’cultural safety’ represents a key philosophical shift from providing care regardless of difference, to care that takes account of peoples’ unique needs”.

What this means is that nurses are no longer required to be colourblind; instead, they must see colour and treat patients differently because of it.
According to the Code, the Board declares, “cultural safety provides a decolonising model of practice based on dialogue, communication, power sharing and negotiation and the acknowledgment of white privilege” (no, I am not making this up — it’s on page 15 of the Code effective 1 March 2018).
The Board decrees that “non-indigenous nurses must address how they create a culturally safe work environment that is free of racism”. Now I know many nurses, including my sister who has spent 20 years working selflessly in indigenous communities, and the idea that they are subtly racist or even insensitive to their patients’ needs is as offensive as the leftist sanctimony that has infected their professional body.

When a body representing some nurses had the temerity to complain about this, Board Chair Associate Professor Lynette Cusack disdainfully replied that it had been endorsed by COAG.
Well, I checked with the Federal health minister Greg Hunt and that’s not accurate. The Minister’s own advice from his Chief Nursing Officer and health department noted that “while the Commonwealth Department of Health provided feedback in the public consultation process, the final changes to cultural safety were made after (this) process. The Department did not see the final version until it was publicly released in March 2018.”
Greg Hunt is one of the smartest politicians I know; I didn’t think he would have let this get through, had he known about it, without a fight.



