“I chose to help create this film because I wanted to help young women living with RHD and make sure they can access information about contraception, pregnancy and planning for a baby.
What is the take home message from the film?
“The film points out the main needs of a young woman living with RHD to help care for herself, her heart and her baby. The film re-assures young women with RHD that they can have a normal healthy pregnancy; they just need to take extra care of themselves.”
RHDAustralia sat down with one of the directors, Ms Kenya McAdam, a 21 year old Jaru and Kira woman from Halls Creek, Western Australia currently living in Katherine, Northern Territory.
See Kenya’s full story PART 2 Below
For Kenya this film was deeply personal and an intimate reflection on life as a young woman living with RHD. Kenya developed RHD at 15 years old and required open heart surgery within 3 months of diagnosis. Since that time, Kenya has worked with RHDAustralia to raise awareness about this 100% preventable disease.
The target audience for this film is girls and young women from ages 13 to 20s who have mild to moderate RHD
“With Aboriginal and Torres Strait Islander Australians still 20 times more likely to die from RHD, the AMA’s call for firm targets and a comprehensive and consultative strategy is welcome. We encourage governments to adopt these recommendations immediately.
“As noted by the AMA, it is absolutely critical that governments work in close partnership with Aboriginal health bodies. Without strong community controlled health services, achieving these targets for reducing RHD will be impossible.
While this is a long term challenge, the human impacts on Aboriginal and Torres Strait Islander communities are being felt deeply right now. Action is required urgently.
NACCHO is standing ready to work with the AMA and governments to develop and implement these measures. We have to work together and we have to do it now.”
National Aboriginal Community Controlled Health Organisation (NACCHO) Chairperson Matthew Cooke pictured above at Danila Dilba Health Service NT with AMA President Dr Michael Gannon
A new film written and directed by a group of Northern Territory Indigenous women follows the story of Tess, a young women whose boyfriend, Jamie, reveals his desire to start a family.
While surprised and happy, she’s not told Jamie about her rheumatic heart disease (RHD).
She’s not sure how her heart disease will affect her pregnancy or if she can have a baby at all. Looking for answers, Tess turns to her best mate, her mum and the local health clinic for guidance on what to do next.
Will they have the answers?
The film will be launched in Bagot Community, Darwin on 6 October. Sharing a Heartbeat is freely available in English and Kriol with plans to make the film available in more Indigenous languages.
You can find these films and other important resources on the RHDAustralia resource page. Additional print resources are linked with the English and Kriol through the resource page on our website.
By embracing two-ways learning and a spirit of cross cultural cooperation, RHDAustralia and Menzies School of Health Research are proud to announce the completion of the first ever educational short film on rheumatic heart disease in pregnancy entitled Sharing a Heartbeat.
Hi Kenya, why did you decide to get involved in the creation of this film?
“I chose to help create this film because I wanted to help young women living with RHD and make sure they can access information about contraception, pregnancy and planning for a baby.
What is the take home message from the film?
“The film points out the main needs of a young woman living with RHD to help care for herself, her heart and her baby. The film re-assures young women with RHD that they can have a normal healthy pregnancy; they just need to take extra care of themselves.”
From a personal perspective, the film answered my unanswered questions. For other young women with RHD, I think it will help them understand more about approaching pregnancy.”
Having Kenya involved from the very start was central to ensuring the film was produced from a patient centric, woman centric and gender sensitive standpoint. But of equal importance was making certain it was developed to be culturally appropriate and safe. This was accomplished by including Indigenous women throughout the process, whether in the design, development, testing or making of the resource.
One of the key contributors alongside Kenya was Noeletta McKenzie whose daughter, Raychelle, was diagnosed with RHD four years ago at the age of nine. Noeletta’s been involved in numerous community development projects in Maningrida and Darwin and was quick to answer a call for assistance with the making of the film. “I saw the advertisement on the RHDAustralia Facebook page and enquired about how I could support with the development of the resource.” Noeletta helped to co-write the film and to guide and consult the actors on set.
When asked about why it was important to have Indigenous women involved in the making of the film she told us “I feel that as the resource is targeted at Indigenous young women, we needed to ensure that they were featured. It’s also about cultural safety and cultural context, educating our young women in our way.”
Leading by example, Noeletta is instilling these qualities into her daughter as well. When asked if the film has helped her daughter learn more about her RHD, Noeletta said “She’s well aware of the disease and how as a young woman it has affected her life. She would like to be a part of an advisory group to share her experience and pass on her knowledge.”
Acknowledgements
There were many people involving in the making of this film and we would like to thank the actors, directors, writers, and producers for producing such a well-crafted and meaningful film that is educational, culturally responsive, collaborative and meaningful. This film was produced by RHDAustralia and made possible with a grant from NTPHN.
Background
Literature reviews and content surveillance of health promotion material from Australia and New Zealand shows that there is very little information available for girls and women who have RHD. A recently completed study conducted by the Australian Maternity Outcomes Surveillance System (AMOSS) has shown that for Indigenous women in Australia, there are many misconceptions around rheumatic heart disease (RHD) and how it can impact their pregnancies.
Films directed by Indigenous women on any content are rare. Rheumatic heart disease is up to twice as common in women, and tends to affect women during their child bearing years. There is a 30-50% increased cardiac workload in normal pregnancy.
The target audience for this film is girls and young women from ages 13 to 20s who have mild to moderate RHD.
Part 2 Rheumatic heart disease a blight on Indigenous population
When Kenya McAdam wasn’t bedridden as a child, she would drag herself to school and sit in the classroom. “I wouldn’t move,” says the 21-year-old childcare worker, whose current good health is proof that she has survived rheumatic heart disease.
But Australia has a high level of the disease, which is caused by a bacterial infection of the throat and skin and is common in poverty-stricken nations.
Some of the nation’s leading medical researchers are meeting today in Darwin to create a plan to wipe out the life-threatening condition, which disproportionately affects indigenous Australians.
Pediatrician Jonathan Carapetis, who has led research efforts for 20 years, says young people such as Ms McAdam are up to 122 times more likely to contract the disease than non-indigenous youngsters. And it affects one in 43 indigenous people living in remote and rural Australia.
“It’s entirely preventable, yet the rates of this devastating condition among Aboriginal and Torres Strait Islander people are among the highest in the world,” says Professor Carapetis, director of Perth’s Telethon Kids Institute. “It should no longer exist in Australia.”
Rheumatic heart disease can result in permanent damage to the heart if it is not treated with antibiotics. It is caused by a bacterial infection of the throat and skin, which can result in heart failure and other complications, including stroke, without antibiotic treatment.
Ms McAdam’s life was saved by heart surgery to repair leaky valves after a cardiac arrest and years of breathlessness. “My mum thought that only older people suffer from heart attacks,” she said.
Her younger brother and sister must endure a painful penicillin injection every month for up to 10 years to prevent further infections.
But many affected indigenous youth fail to receive more than half their monthly penicillin requirement. More than 2600 people in the Northern Territory have rheumatic heart disease, while sufferers in Western Australia’s remote Kimberley Region are recorded as dying at an average age of 41.
Professor Carapetis said research institutes around Australia were collaborating on ways to prevent and treat streptococcus infections that lead to the disease, such as long-acting penicillin or an antibacterial vaccine.
Heather D’Antoine, from Menzies School of Health Research’s Aboriginal Programs, said today’s meeting to discuss lifesaving initiatives “can’t come soon enough”.
“The impact on our community is devastating; children must travel for heart surgery; young adults live with premature disability; and pregnant women face high-risk pregnancies,” she said.
Wednesday by 4.30 pm for publication each Thursday
1.1 NACCHO CEO Pat Turner to build on the success of Aboriginal Community Control Health Services
Pat Turner has been appointed for a further three years until July 2020 by the National Aboriginal Community Controlled Health Organisation (NACCHO) Board.
NACCHO Deputy Chairperson, Sandy Davis welcomed Ms Turner’s appointment highlighting her extensive life experiences in Aboriginal affairs, government, academia and corporate practice.
Sandy also ‘acknowledged her invaluable record of public service achievements and that her leadership style comes at an important time for NACCHO with new governance arrangements to be discussed with members’ at our Annual General Meeting in Canberra in November.
Pat will help create real, meaningful and lasting change for NACCHO that will strengthen community control and keep Aboriginal health in Aboriginal hands’ he said.
Pat recently finalised a new network funding agreement for supporting community controlled Aboriginal health service with the Commonwealth. This will allow for better, more targeted investment in efforts to close the health gap for Aboriginal people. Pat has consistently said that ‘governments at all levels must do more to join the dots between education, housing, employment and other social determinants if we are to significantly improve health outcomes for our people and Close the Gap they have spoken about for the best part of a decade.’
Pat has been delivering on the Board’s agenda to consult with members to update our NACCHO Constitution and she has spent the last few months criss-crossing Australia to obtain the views and opinions of our Members and Affiliates about NACCHO constitutional changes.
She will continue to work on strengthening and expanding the Aboriginal Community Controlled Health Sector, maintaining its strategic directions, cutting unnecessary red tape and building a closer relationship between all our organisations. ‘We want to build on the success of community control in improving health outcomes for our people’ she said.
Pat is of Arrernte and Gurdanji descent and was awarded the Order of Australia (AM) in 1990 for her contribution to public service.
1.2 National : 2017 NACCHO Members’ Conference and AGM Registrations : Only 28 days to go
On Tuesday 2 October there was only 28 days to go and due to high demand the conference AGM is nearly booked out
This is an opportunity to show case grass roots best practice at the Aboriginal Community Controlled service delivery level.
In doing so honouring the theme of this year’s NACCHO Members’ Conference ‘Our Health Counts: Yesterday, Today and Tomorrow’.
These girls and boys are representing the Healthy Lifestyle Values and doing us proud today! Well done everyone on being deadly team players and making healthy choices!
Check out their other healthy lifestyle tips below. HERE
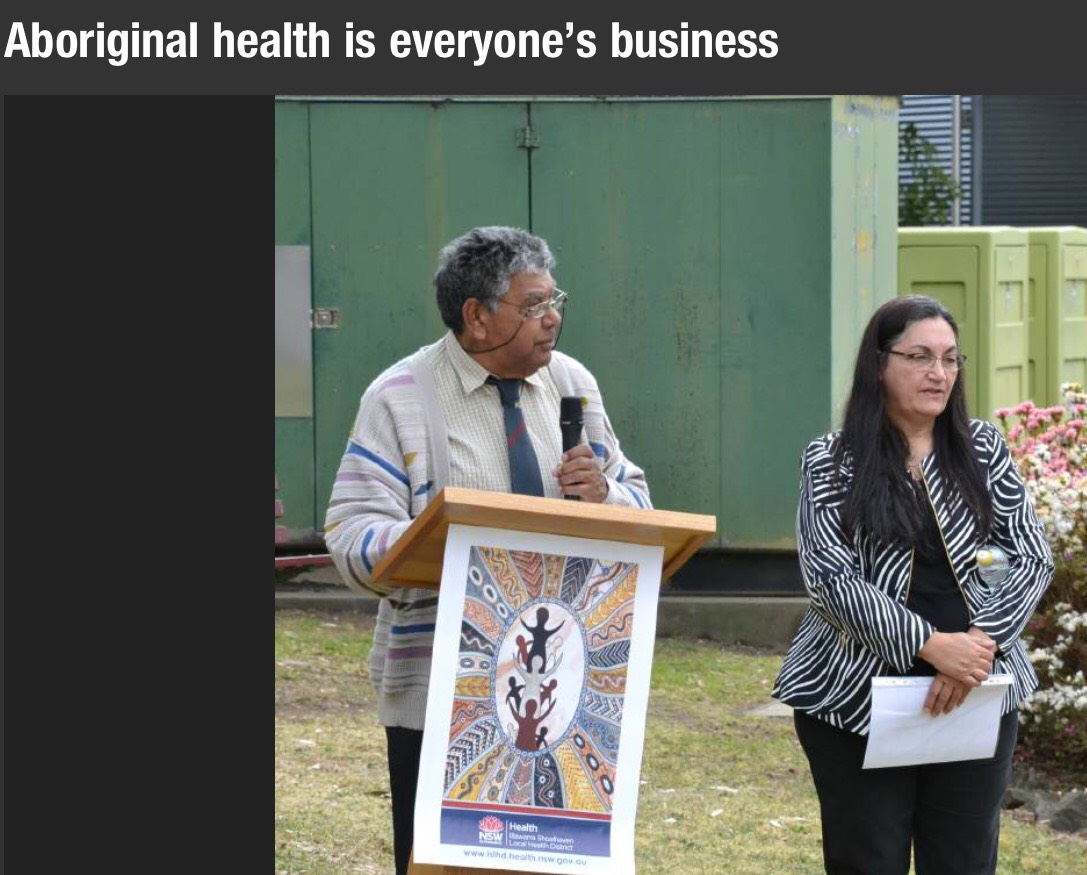
3.NSW : In the Shoalhaven region Aboriginal Health is everyone’s business
Illawarra Shoalhaven Local Health District (ISLHD) has joined local Aboriginal Community Controlled Health Services, the Primary Health Network and the University of Wollongong in committing to work together to bring about positive changes to Close the Gap on health inequalities for our Aboriginal communities.
A partnership agreement was formally signed on Friday by leaders of the South Coast Aboriginal Medical Service; Oolong House – Drug and Alcohol Rehabilitation Centre; Illawarra Aboriginal Medical Service; Waminda South Coast Women’s Health and Welfare Aboriginal Corporation; University of Wollongong; COORDINARE – South Eastern NSW Primary Health Network; and Illawarra Shoalhaven Local Health District.
A special ceremony, including a corroboree, smoking ceremony and performances by the Doonooch Dancers led by Joe Brown-McLeod and Larry McLeod,
and a stirring welcome to country by Uncle Tom Moore preceded the official signing of the agreement.
ISLHD Chief Executive Margot Mains said the agreement aims to support, promote and strengthen the existing local relationships and strong ties that have been developed over many years.
“The signing of the partnership agreement marks a new beginning for our journey in working collaboratively to close the health and life expectancy gap between Aboriginal people and non-Aboriginal Australians,” Ms Mains said.
4.NT : Ken Wyatt opens our NACCHO #OchreDay2017 summit in Darwin
Losing his nephew to the same preventable disease that afflicts so many Aboriginal Australians galvanised Ken Wyatt to make indigenous men’s health a “top priority” of his political agenda.
The Federal Indigenous Health Minister says his nephew was a promising musician but died in June, aged just 35, after a battle with diabetes and chronic renal and heart disease.
“One of Jason’s killers was kidney failure, the same devastating condition that claimed the life of beloved musician, Dr G Yunipingu,” Mr Wyatt told a national men’s health conference in Darwin.
“His close family and friends are now working on a media project to fulfil his dying wishes – to get the word out to indigenous men in particular, to take their health seriously, to own it.”
Aboriginal men have the poorest health of any group within the Australian population, which Mr Wyatt says is “nothing short of a national tragedy”.
They suffer kidney health problems at five times the rate of their non-indigenous counterparts, and are dying more than 10 years younger.
Winner of the Jaydons Adams Award
From the left, Mr Mark and Mrs Lizzie Adams with Nathan Cubillo-Jones and AMSANT CEO John Paterson
He’s just graduated this year from his studies as an Indigenous health practitioner and in between playing local Aussie rules and Rugby league, he worked tirelessly with Danila Dilba health service and has recently been appointed manager of the new Malak clinic.
5. QLD : Inquiry into service delivery in remote and discrete Aboriginal and Torres Strait Islander communities : Draft report consultation
The draft report is scheduled to be released in early October 2017.
We are seeking your comments and views on the draft report, and will be undertaking further consultation during October and early November.
The Commissioner Bronwyn Fredericks will be briefing and consulting with stakeholders in the following locations:
9 October 2017 (1pm to 3pm) – Cairns, Doubletree Hilton Hotel
10 October 2017 – Yarrabah
11 October 2017 – Kowanyama
12 October 2017 – Lockhart River
13 October 2017 – Aurukun
16 October 2017 – Gladstone (LGAQ conference)
17 October 2017 – Woorabinda
20 October 2017 – Brisbane
Further consultations will be scheduled in the coming weeks at Mt Isa, Mornington Island, and Thursday Island – details will be published on the QPC website as they become available.
Consultations will include round tables in Cairns, Mt Isa, Thursday Island and Brisbane.
Please register your interest to attend a consultation or round table here.
If you would like to meet with the Commissioner or the inquiry team either as part of the consultation rounds or via teleconference, please contact us on (07) 3015 5111 or enquiry@qpc.qld.gov.au
6.ACT : NACCHO/WinnungaNimmityjah Aboriginal Health Service mental health webinar in conjunction with the Mental Health Professionals Network
On Wednesday the 13th of September 2017, NACCHO facilitated a mental health webinar in conjunction with the Mental Health Professionals Network as part of its professional development work.
This mental health webinar focused on reducing the mental health impacts of indigenous incarceration on people, communities and services.
The discussion was conducted by an Indigenous interdisciplinary panel (see below for further details). A post-discussion Q&A was also conducted between the panel and guests, recordings of which can be accessed below.
THE PANEL
Julie Tongs OAM (CEO Winnunga Nimmityjah Aboriginal Health Service)
Dr Louis Peachey (Rural Generalist)
Dr Marshall Watson (Psychiatrist)
Dr Jeff Nelson (Psychologist)
Facilitator: Dr Mary Emeleus (General Practitioner and Psychotherapist).
7.WA : Puntukurnu Aboriginal Medical Service’s Tackling Indigenous Smoking team to create Anti Smoking Ads
The project, organised by Puntukurnu Aboriginal Medical Service’s Tackling Indigenous Smoking team, will be carried out with funding from a Healthway Indigenous Health Promotion grant and the Federal Government’s Tackling Indigenous Smoking Program.
Puntukurnu Aboriginal Medical Service regional tobacco coordinator Danika Tager said smoking rates in the East Pilbara were exceptionally high and more needed to be done to support communities to address tobacco addiction.
Filmmakers will work with youth in four remote Aboriginal communities in the East Pilbara to shed light on the personal stories of local smokers and warn about the perils of the deadly habit.
Young people, assisted by a professional production team, will create a series of short films as part of the “you CAN quit” project, to document the stories of community members who have successfully kicked the habit and those who have been affected by smoking-related illnesses in Jigalong, Parnngurr, Punmu and Kunawarritji.
Statistics from the Federal Department of Health show that tobacco smoking is responsible for one in five Aboriginal and Torres Strait Islander deaths, with the number substantially higher in remote areas.
“Smoking rates in remote East Pilbara communities are as high as 80% and tobacco use is the single most preventable cause of death and disease in this population,” Ms Tager said.
“Through this important film project we hope to encourage people in these communities to quit smoking, as well as air the many benefits of quitting and where they can find help and support.”
Filming of the four short films will start September 19. It is expected the films will be screened in each community on completion and also be aired on indigenous television stations and social media.
Ms Tager said the project was unique in that the films would be entirely community owned and directed, giving young people the opportunity to actively make a difference in their community.
“Youth will be responsible for all aspects of researching, shooting, editing and promoting the films” she said.
“All too often NGOs will come into a community with a health message that may or may not be relevant, and expect it to change people’s behaviour,” she said.
“What we are doing here is empowering the community to send its own messages and fight tobacco-related harm using its own experience and stories.”
The project will also involve a series of posters to celebrate non-smokers in the communities, and offer education sessions and details about the availability of support programs.
The Puntukurnu Aboriginal Medical Service (PAMS) is a community controlled health organisation that provides primary health care, 24-hour emergency services and preventative health and education programs in the communities of Jigalong, Parnngurr, Punmu and Kunawarritji.
8. Tas : Tasmanian Aboriginal Centre to celebrate our communities journey of breast cancer & raise awareness
Please join us at piyura kitina (Risdon Cove) on Thursday, 12th October at 1.30pm, to celebrate our communities journey of breast cancer & raise awareness of this disease.
Afternoon tea, will be provided, please contact Emma on
6234 0777 or Freecall 1800 132 260 if you require transport.
9.SA : Aboriginal Health Council of SA and South Australian Aboriginal Chronic Disease Consortium
The South Australian Aboriginal Chronic Disease Consortium (the Consortium) was launched on 18 May 2017, as a collaborative partnership formed between the South Australian Aboriginal Health Partnership (comprising of SA Health, Aboriginal Health Council of SA and Department of Health – Commonwealth) and the South Australian Academic Health Science and Translation Centre.The Translation Centre represents a partnership between SA Health, South Australian Health and Medical Research Institute (SAHMRI), University of Adelaide, Flinders University, University of South Australia, Aboriginal Health Council of South Australia, Health Consumers Alliance of South Australia, Adelaide Primary Health Network, Country SA Primary Health Network and Cancer Council SA. The Translation Centre has 9 priority areas of which one is Aboriginal Health.
Consortium Vision
The Consortium’s vision is to reduce the impact of chronic disease experienced by Aboriginal and Torres Strait Islander people living in South Australia through the successful implementation of the priorities identified within 3 plans: The South Australian Aboriginal Cancer Control Plan 2016-2021, the South Australian Aboriginal Heart and Stroke Plan 2017-2021 and the South Australian Aboriginal Diabetes Strategy 2017-2021.How will the Consortium Work
The responsibility to oversee the implementation activity of the SA Aboriginal Chronic Disease Consortium rests within its governance structures. The Consortium has 5 active working groups including an Executive Group, an Aboriginal Community Reference Group and three condition-specific leadership groups representing Diabetes, Cancer and Heart and Stroke. We refer to the people and organisations on these groups as our members.
Who is working in the Consortium Coordinating Centre?
The team comprises of two full time staff. Wendy Keech is the Senior Research Translation Manager and Executive Officer. Wendy is supported by Douglas VJ Clinch, in a Project Officer role overseeing and supporting the various governance groups of the Consortium. Strategic policy and cultural advice and support is being provided by Kim Morey and Neville Fazulla both on a part-time basis to the team, and have particular focus on supporting the community reference group. Andrea McKivett, has been providing her clinical, technical and cultural support to the team since the inception of the Consortium, with Katharine McBride recently joining the team to provide technical support one day a week. The team come from various backgrounds and disciplines required to support the work of the Consortium, and all are passionate people with a strong commitment to making a difference to the health and wellbeing of Aboriginal people in South Australia.
If you would like any further information please don’t hesitate to contact Wendy Keech, on (08) 81284228, email: wendy.keech@sahmri.com or Doug VJ Clinch, on (08) 81284893 or email: douglas.clinch@sahmri.com.
In 2017, around 373,000 Australian males (3.1%) identified as Aboriginal and/or Torres Strait Islander [1, 2]. Indigenous males tend to be younger than non-Indigenous males (34% aged less than 15, compared with 19% of non-Indigenous males), they are culturally diverse (17% speak an Indigenous language and 61% identify with a clan, tribal or language group) and they are outnumbered by females in later life (85 males for every 100 females aged 65 or over) [2, 3].
NACCHO has long recognised the importance of an Aboriginal male health policy and program to close the gap by 2030 on the alarming Aboriginal male mortality rates across Australia.
Aboriginal males have arguably the worst health outcomes of any population group in Australia.
To address the real social and emotional needs of males in our communities, NACCHO proposes a positive approach to Aboriginal male health and wellbeing
NACCHO, its affiliates and members are committed to building upon past innovations and we require targeted actions and investments to implement a wide range of Aboriginal male health and wellbeing programs and strategies.
We call on State, Territory and Federal governments to commit to a specific, substantial and sustainable funding allocation for the NACCHO Aboriginal Male Health 10 point Blueprint 2013-2030
Who are Australia’s males?
As at June 30 2016, there were nearly 12 million males living in Australia (49.7% of the total population), which means there were 98.8 males for every 100 females [1]. Most males (68%) were younger than 50 and 14% were 65 or over. Their median age was 36.5 years, which is lower than the median age for females of 38.3 years.
Males are a diverse population, with differing health behaviours, conditions and health service use across a range of characteristics. The characteristics of five particular population groups are described below.
Remoteness
From the 2011 ABS census, 69% of the Australian male population live in Major cities, 19% live in Inner regional areas, 9.3% live in Outer regional areas, and 2.5 per cent live in Remote and Very remote areas [4]. Males living in Remote and Very remote areas outnumber females (116 males for every 100 females) and are community-minded (19% volunteer for a group or organisation, compared with 14% of males living in Major cities)[4].
Socioeconomic disadvantage
Some Australian males are more disadvantaged than others. Thirteen per cent of males are experiencing poverty and around 59,000 are homeless [5, 6]. There are nearly 36,000 Australian male prisoners in adult corrective services custody [7]. Two out of three (66%) males aged 15 and over are employed and 60% of 15–74 year old males have a non-school qualification [8, 9].
Region of birth
More than a quarter (27%) of the Australian male population were born overseas. Of those born overseas, the majority were born in the United Kingdom (followed by New Zealand and China), and overseas-born males are outnumbered by overseas-born females (98 males for every 100 females) [10].
Age group
In 2016, 23% of the total male population were aged under 18, 62% were aged 18–64, and 14% were aged 65 or over [1]. The number of men aged 65 and over is increasing (by the year 2026 they are predicted to account for 17 to 18% of the total male population), they are outnumbered by females (88 males for every 100 females), 11% are widowed, 17% live alone, and 16% need assistance with one or more of the core everyday activities of self-care, mobility and communication [11].
Lifestyle and risk factors of Australia’s males
The lifestyles males lead can influence how healthy they are in the short and long term. A lifestyle including exercise, a well-balanced diet, and maintaining a healthy body weight, may reduce the risk of poor health. Risk factors such as smoking tobacco, misusing alcohol and illicit substance use, or exposure to violence, may increase the likelihood of poor health.
Physical activity
Regular physical activity helps maintain a healthy body weight and reduce the risk of many chronic conditions and injuries. Sport and other forms of physical activity can also improve mental wellbeing and may foster social networks which provide support and opportunities for development.
Sufficient physical activity for 18–64 year olds is defined in Australia’s Physical Activity & Sedentary Behaviour Guidelines as accumulating at least 150 minutes of moderate physical activity every week, and being active on most, preferably all, days. The guidelines also recommend adults complete at least two strength-based training sessions each week. The guidelines provide separate recommendations for children (ages 0–5 and 5–12), young people (ages 13–17), and older Australians (ages 65+).
In this section, we refer to ‘sufficient activity’ for 18–64 year olds as completing at least 150 minutes of physical activity across 5 or more sessions each week. For males aged 65 and over, ‘sufficient activity’ is completing at least 30 minutes of exercise on most days each week (reported here as 5 or more days).
1 in 2 Australian men aged 18–64 get enough exercise
In 2014–15, 49% of men aged 18–64 exercised sufficiently [1]. Exercise rates were highest among men aged 25–34 (56%) and lowest among men aged 45–54 (43%).
1 in 4 (27%) men aged 65 and over were sufficiently active.
Figure 1: Sufficient physical activity, men aged 18–64, by age-group, 2014-15
Note: “Sufficiently active” here refers to having completed at least 150 minutes of physical activity over 5 or more sessions in the previous week.
Excess body weight, known as overweight and obesity, is a risk factor for many conditions, including cardiovascular disease, high blood pressure, Type 2 diabetes, sleep apnoea and osteoarthritis. Excess body weight can be measured using the body mass index (BMI).
7 in 10 Australian men are overweight or obese
In 2014–15, 7 in 10 adult males in Australia (71%) were overweight or obese: 42% were overweight, and 28% were obese [1]. The proportion of males who are overweight or obese differs by population group [1, 2, 3]:
44% of young men (aged 18–24) are overweight or obese, compared with 82% of men aged 55–64
the rate of overweight and obesity in men does not vary substantially across areas of socioeconomic disadvantage, ranging from 69% to 73%
75% of men living in Inner regional areas are overweight or obese, compared with 69% of men living in Major cities
38% of Aboriginal and Torres Strait Islander men were obese in 2012–13, compared to 27% of non-Indigenous men, after adjusting for differences in age-structure. However, the overall rate of overweight and obesity was the same (70% for both).
The proportion who are overweight or obese differs between boys and men, 7 in 10 (71%) men aged 18 years and over are overweight or obese, compared with 3 in 10 (28%) boys aged 5–17.
Figure 2: BMI, boys aged 5–17 and men aged 18 and over, 2014–15
While excess weight is commonly managed using dietary intervention and exercise, for those who are morbidly obese or who are obese and have other conditions related to their excess weight, weight loss surgery may be appropriate.
Weight loss surgery (bariatric surgery) is surgery that aims to help obese patients lose weight and lower the risk of medical problems associated with obesity. It restricts the amount of food a recipient can eat or alters the process of food digestion so that fewer calories are absorbed.
In 2014–15, males accounted for 21% of hospital separations for weight loss surgery (4,800 separations) compared to 79% for females (18,000 separations) [4].
Tobacco smoking is the single most preventable cause of poor health and death in Australia [5]. The main data sources reporting on tobacco smoking in Australia are the ABS National Health Survey’s (NHS), the National Australian Aboriginal and Torres Strait Islander Social Survey, and the AIHW National Drug Strategy Household Survey (NDSHS).
These surveys showed that:
based on the ABS NHS, in 2014–15, 16.9% of men aged 18 or over and 3.9% of boys aged 15–17 years smoked daily [1]
based on the AIHW NDSHS, in 2016, 14.6% of men aged 18 or over and 2.7% of males aged 14–19 smoked daily [6].
The proportion of males who smoke tobacco differs by age and between population groups [1, 3, 7]:
19.4% of younger men (aged 18–44) smoked daily, compared with 14.6% of older men (aged 45 or over)
24.6% of men living in the lowest socioeconomic areas smoked daily, compared with 8.7% of men living in the highest socioeconomic areas
25.0% of men living in Outer regional and remote areas smoked daily, compared with 15.5% of men living in Major cities
43.9% of Aboriginal and Torres Strait Islander men smoked daily in 2014–15, compared to 17.0% of non-Indigenous men, after adjusting for differences in age-structure.
Alcohol
Excessive alcohol consumption is a major risk factor for a variety of health problems, including liver and heart conditions, and poor mental health. It also contributes to accident and injury, such as motor vehicle accidents, physical violence and homicide. The main data sources reporting on alcohol consumption in Australia are the AIHW National Drug Strategy Household Survey and the ABS National Health Survey. Although these surveys use different methodologies, they show similar results.
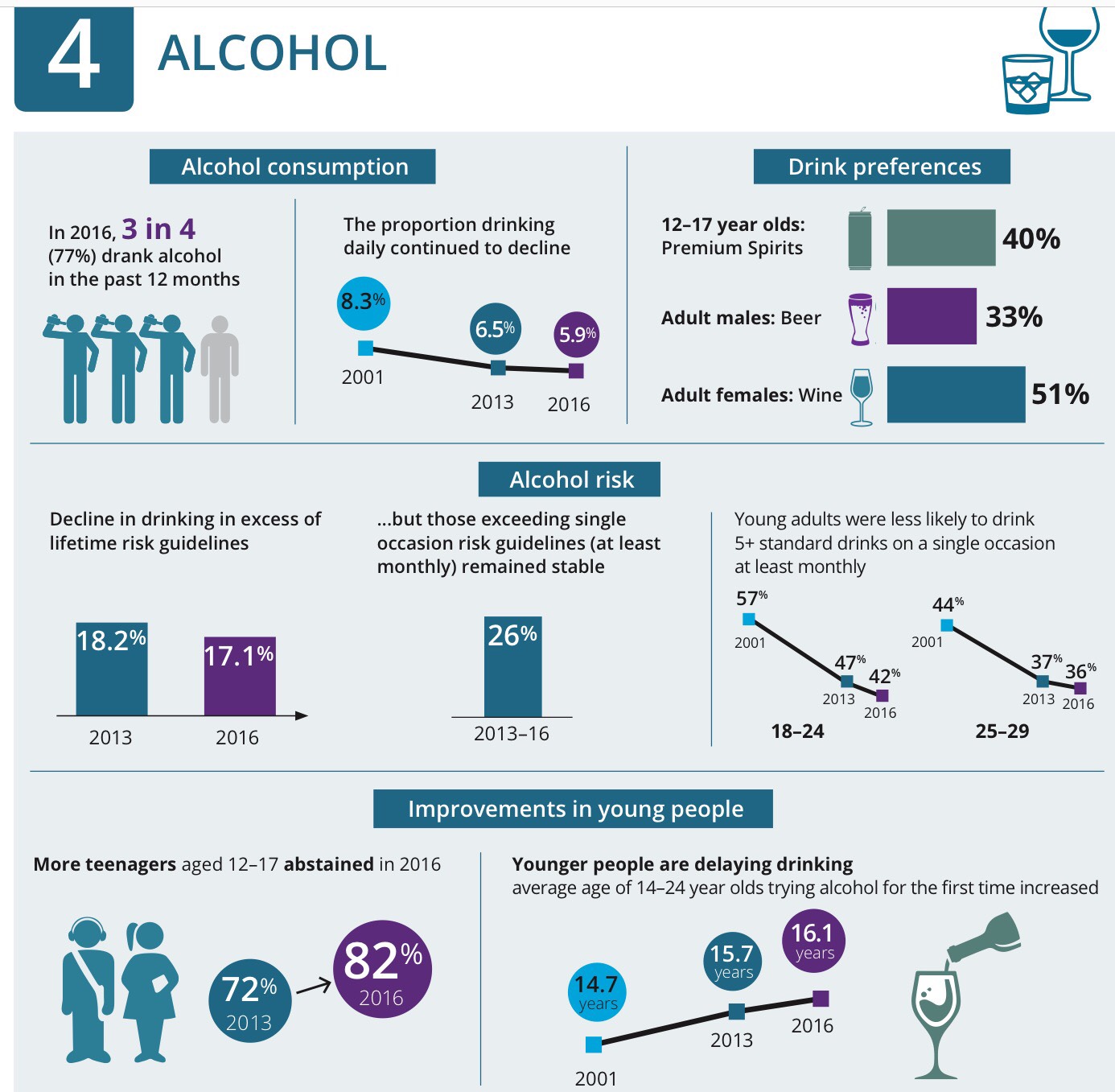
Based on the AIHW NDSHS, in 2016 26% of men (ages 18+) were lifetime risky drinkers [6]. Half of men aged 18 and over (49%) exceeded the single occasion risky drinking threshold at least once in the last 12 months.
Based on the ABS NHS, in 2014–15, more than half of men aged 18 and over (57%) were exceeding the single occasion risk threshold, and one in four (26%) exceeded the lifetime risk guideline. The rates of lifetime and single occasion risky drinking vary by age-group (see Figure 3) [1].
Figure 3: Lifetime and single occasion risky drinking, men, by age-group, 2014–15
Lifetime risky drinking
Single occasion risky drinking
Note: Alcohol consumption risk levels based on 2009 National Health and Medical Research Council (NHMRC) guidelines for the consumption of alcohol.
The proportion of men who exceed the lifetime alcohol risk guidelines varies by age and between population groups [1, 2, 3]:
19% of younger men (aged 18–24) exceed the lifetime alcohol risk guidelines, compared with 31% of men aged 55–64
23% of men living in the lowest socioeconomic areas exceed the lifetime alcohol risk guidelines, compared with 29% of men living in the highest socioeconomic areas
37% of men living in Outer regional and remote areas exceed the lifetime alcohol risk guidelines, compared with 24% of men living in Major cities
Aboriginal and Torres Strait Islander men had the same rates of risky drinking as non-Indigenous men in 2012–13, with 29% of both groups exceeding the lifetime alcohol risk guidelines, after adjusting for differences in age-structure.
Illicit substances
Illicit substance use includes the use of illegal drugs (such as cannabis and heroin), or inappropriate use of prescription pharmaceuticals (such as sleeping pills) or other substances (such as naturally occurring hallucinogens). Illicit use of drugs causes death and disability and is a risk factor for many diseases. The effects of illicit drug use can be severe, for example leading to poisoning, heart damage, mental illness, self-harm, suicide and death. Illicit drug use is also associated with risks to users’ families and friends and to the community. It contributes to social and family disruptions, violence, and crime and community safety issues. The AIHW National Drug Strategy Household Survey reports on illicit drug use in Australia.
In 2016, 18% of Australian males aged 14 years and over had used an illicit drug in the previous 12 months (‘recent use’) [6].
The pattern of illicit substance use differs by age groups—32% of men aged 20–29 had recently used illicit drugs, compared with 7.9% of men aged 60 or over.
Violence
Violence is the intentional threat or actual use of physical force or power against oneself, another person, or a group, that results in injury, death, psychological harm, abnormal growth or deprivation. The main data source for violence is the ABS Personal Safety Survey.
1 in 2
Australian men have experienced violence since they turned 15
In 2012, for men aged 18 or over [8]:
49% had experienced violence since the age of 15—48% had experienced physical violence and 4.5% had experienced sexual violence
8.7% had experienced violence in the last 12 months, with the highest rates for men aged 18–24 (24%), and the lowest for men aged 55+ (2.2%)
5.3% had experienced partner violence since the age of 15
7.8% had been stalked in their lifetime
14% had experienced emotional abuse by a partner since the age of 15
18% had experienced sexual harassment during their lifetime.
How healthy are Australia’s males?
A person’s health status is their overall level of health, and can be measured through self-assessed health status; presence of chronic disease and comorbidities; mental health; sexual heath; life expectancy; and level of disability.
Self-assessed health status
Self-assessed health status is a general measure of health status, combining physical, social, emotional and mental health and wellbeing.
Nearly 3 in 5
Australian males rated their health as excellent or very good
In 2014–15, 55% of males (aged 15+) rated their health as excellent or very good [1].
The proportion of males rating their health as excellent or very good varied by age-group: 64% of males aged 15–34 rated their health as excellent or very good, compared with 32% of men aged 75 years and over.
Chronic disease, comorbidity and burden of disease
Chronic disease
The term chronic disease applies to a group of diseases that tend to be long-lasting and have persistent effects. Chronic diseases have a range of potential impacts on a person’s individual circumstances, including quality of life, as well as broader social and economic effects. Chronic diseases also have a significant impact on the health sector.
Self-reported data from the Australian Bureau of Statistics (ABS) 2014–15 National Health Survey (NHS) provides an estimate of the prevalence of chronic disease among the Australian population. Chronic disease data is collected for arthritis, asthma, back problems, cancer, COPD (chronic obstructive pulmonary disease), CVD (cardiovascular disease), diabetes, and mental health conditions. These chronic diseases were selected for reporting because they are common, pose significant health problems, have been the focus of recent AIHW surveillance efforts, and action can be taken to prevent their occurrence. This survey data is self-reported and is therefore likely to under-report the true prevalence of chronic disease. However, using this data enables us to look at the comorbidity of chronic diseases across the Australian population, which is not possible using separate data sources. For more information on data quality see Data sources.
1 in 2 Australian males have a chronic disease
In 2014–15, 48% of males reported having one or more of the 8 selected chronic diseases (arthritis, asthma, back problems, cancer, cardiovascular disease, COPD, diabetes and mental and behavioural problems) [1].
Table 1: Selected chronic diseases reported by males, all ages, 2014–15
Condition
Number
Per cent
Condition
CVD (cardiovascular disease)
Number
2,042,700
Per cent
17.9
Condition
Back problems
Number
1,851,900
Per cent
16.2
Condition
Mental and behavioural problems
Number
1,803,400
Per cent
15.8
Condition
Arthritis
Number
1,409,000
Per cent
12.3
Condition
Asthma
Number
1,119,800
Per cent
9.8
Condition
Diabetes
Number
647,100
Per cent
5.7
Condition
COPD (chronic obstructive pulmonary disease)
Number
301,500
Per cent
2.6
Condition
Cancer
Number
195,500
Per cent
1.7
Source: ABS 2015 [1]
Note: This survey data is self-reported and likely under-reports the true prevalence of chronic diseases. For more information on data quality see Data sources.
The prevalence of these chronic diseases varies with age:
86% of men aged 65 and over have a chronic disease, compared with 33% of males aged under 45.
Cancer
Cancer describes a diverse group of several hundred diseases in which some of the body’s cells become abnormal and begin to multiply out of control. Some cancers are easily diagnosed and treated, others are harder to diagnose and treat, and all can be fatal. Cancers are named by the type of cell involved or the location in the body where the disease begins.
The primary source of national cancer incidence data is the Australian Cancer Database – a data collection of all primary, malignant cancers diagnosed in Australia since 1982.
16,665
Estimated new cases of prostate cancer will be diagnosed in 2017, the most common cancer among males
In 2017, it is estimated males will account for 54% of all new cancer cases (72,169 cases) [2]. The risk for Australian males of being diagnosed with cancer before their 85th birthday is 1 in 2 (see Figure 4 below). The most common cancer diagnosis in males is prostate cancer, followed by colorectal cancer, melanoma of the skin, and lung cancer.
Figure 4: Estimated age-specific incidence and mortality rate from all cancers, males, 2017
The World Health Organisation defines mental health as ‘a state of wellbeing in which every individual realises his or her own potential, can cope with the normal stresses of life, can work productively and fruitfully and is able to make a contribution to her or his community.’ Poor mental health may adversely affect any or all of these areas and has consequences for an individual, their family and society.
Nearly 1 in 2
Australian males have experienced a mental health problem
In 2007, more than 3.8 million (48%) males aged 16–85 had experienced a mental health disorder in their lifetime [3].
18% of males aged 16–85 experienced symptoms of a mental health disorder in the previous 12 months.
Chronic disease comorbidities
Some people have more than one chronic disease or health problem at the same time. This is referred to as a comorbidity. Having comorbid chronic conditions can have important implications for a person’s health outcomes, quality of life and treatment choices.
Comorbidity data are presented for the following eight chronic diseases because they are common, pose significant health problems, have been the focus of recent AIHW surveillance efforts, and action can be taken to prevent their occurrence:
arthritis
asthma
back problems
cancer
COPD (chronic obstructive pulmonary disease)
CVD (cardiovascular disease)
diabetes
mental health conditions.
In 2014–15, 48% of all Australian males had one or more of these chronic conditions: 27% had one, 13% had two, and 8.5% had three or more. Chronic disease comorbidity was lower for males than females (21% of all males had two or more chronic conditions compared with 25% for females). [1]
Figure 5: Number of chronic conditions, males, 2014–15
Note: Based on the selected chronic conditions; arthritis, asthma, back pain and problems, cancer, cardiovascular disease, chronic obstructive pulmonary disease, diabetes, and mental health conditions.
717,300 males reported CVD and arthritis (6.3% of all males)
580,100 males reported CVD and back problems (5.1%)
509,300 males reported mental and behavioural problems and back problems (4.5%).
Burden of disease
Burden of disease quantifies the health impact of disease on a population in a given year—both from dying early and from living with disease and injury. The summary measure ‘disability-adjusted life years’ (or DALY) measures the years of healthy life lost from death and illness.
In 2011, males experienced a greater share of the total disease burden (54%) than females (46%) [4]. The distribution of overall burden between the sexes varied by disease group. Compared with females, males experienced almost three-quarters (72%) of the total burden from injuries and a greater proportion of the total burden from cardiovascular diseases (59%). Nearly half (47%) of the burden of disease in males is from cancer, cardiovascular disease, and mental & substance use disorders.
After cancer, the ranking of disease groups contributing to total burden of disease differed for males and females. For males, cardiovascular diseases ranked second, followed by mental & substance use disorders, injuries, and musculoskeletal conditions (see Table 2). For females, musculoskeletal conditions ranked second, followed by cardiovascular diseases, and mental & substance use disorders [4].
Table 2: Leading causes of burden, DALY and proportions, by disease group, males, 2011
Disease group
DALY
Proportion (%)
Disease group
Cancer
DALY
470,110
Proportion (%)
19.5
Disease group
Cardiovascular
DALY
388,306
Proportion (%)
16.1
Disease group
Mental & substance use disorders
DALY
283,652
Proportion (%)
11.8
Disease group
Injuries
DALY
283,228
Proportion (%)
11.7
Disease group
Musculoskeletal
DALY
232,044
Proportion (%)
9.6
Disease group
Respiratory
DALY
184,297
Proportion (%)
7.6
Disease group
Neurological
DALY
128,273
Proportion (%)
5.3
Disease group
Gastrointestinal
DALY
78,839
Proportion (%)
3.3
Disease group
Infant/congenital
DALY
68,212
Proportion (%)
2.8
Disease group
Endocrine
DALY
60,587
Proportion (%)
2.5
DALY = Disability Adjusted Life-Year.
Source: AIHW 2015 [4]
Sexual health
Sexual health includes the prevalence of sexual problems and sexually transmissible infection rates.
Over 1 in 2 Australian men have experienced a sexual difficulty
More than half (54%) of men aged 18–55 years had experienced some sexual difficulty lasting at least 3 months in the last 12 months: 37% ‘came to orgasm too quickly’ and 17% ‘lacked interest in sex’ [5].
‘Reaching climax too quickly’ was the most common issue across all age groups (between 32% and 38%). Other types of sexual difficulty differed by age: ‘did not reach climax or took a long time’ was the next most common issue in 18–24 year old men, while ‘lacking interest in having sex’ was most common among men of other age groups (25–34, 35–44 and 45–55).
Table 3: Sexual difficulty among men, by age group, 2013–14
Age group (years)
Sexual difficulty (a)
Per cent (b)
18–24
Reached climax too quickly
31.5
Did not reach climax or took a long time
16.8
Lacked interest in having sex
14.6
At least one sexual difficulty over past 12 months
48.3
25–34
Reached climax too quickly
36.3
Lacked interest in having sex
15.1
Felt anxious during sex
10.2
At least one sexual difficulty over past 12 months
51.6
35–44
Reached climax too quickly
39.2
Lacked interest in having sex
16.7
Did not reach climax or took a long time
13.8
At least one sexual difficulty over past 12 months
54.2
45–55
Reached climax too quickly
38.0
Lacked interest in having sex
20.2
Had trouble getting or keeping an erection
19.9
At least one sexual difficulty over past 12 months
56.6
Sexual difficulty experienced for at least three months in the 12 months before the study.
Proportion of males in each age group. Note that males may report more than one sexual difficulty.
Source: [5]
Life expectancy and mortality
Life expectancy is expressed as either the number of years a newborn baby is expected to live, or the expected years of life remaining for a person at a given age, and is estimated from the death rates in a population.
Australian males born in 2013–15 can expect to live 33 years longer than males born in 1881–1890 did
Life expectancy changes over time, and differs between population groups [6, 7]:
males born in Australia in 2013–2015 can expect to live to the age of 80.4 years on average
for Aboriginal and Torres Strait Islander males born in 2010–2012, life expectancy was estimated to be 10.6 years lower than that of non-Indigenous males (69.1 years compared with 79.7)
Australia is ranked 7th in international comparison of life expectancy at birth for males at 80.3 years, Iceland is ranked 1st with 81.3 years.
Disability-free life expectancies
Life and health expectancies at age 65 are used for monitoring healthy ageing. In 2013–15, life expectancy for men aged 65 (that is, the number of additional years a person aged 65 could expect to live) was just under 20 years [6]. Men aged 65 in 2015 could expect to live an additional 9 years free of disability and around 10 years with some level of disability, including 3 years with severe or profound core activity limitation. This equates to these men living 53% of their remaining life with disability, including 17% with severe or profound core activity limitation [7].
Mortality
Mortality data, such as premature deaths and potentially avoidable deaths, can help in understanding death and the fatal burden of disease in the population at a point in time.
Mortality rates vary between population groups. In 2015 [8]:
Males accounted for 62% of premature deaths.
Males in Very remote areas had a higher percentage of potentially avoidable deaths, with 61% of premature deaths being potentially avoidable, compared to 50% in Major cities
The median age at death for males decreased with increasing remoteness: from 79 in Major cities to 67 in Very remote areas
The median age at death for males also decreased with decreasing socioeconomic group: from 81 in the highest socioeconomic areas to 77 in the lowest socioeconomic areas
Causes of death
Monitoring causes of death helps to measure the health status of a population. Causes of death can be used to assess the success of interventions to improve disease outcomes, signal changes in community health status and disease processes, and highlight inequalities in health status between population groups.
In 2015, there were 81,330 deaths among Australian males. The leading cause of death was coronary heart disease, followed by lung cancer and dementia & Alzheimer disease. Males had over three times the rate of suicide and nearly twice the rates of death from coronary heart disease and lung cancer as females when adjusted for differences in the age structure of the populations.
Figure 6: Leading causes of death among males, 2015
Notes:
Data are based on year of registration of death; deaths registered in 2015 are based on the preliminary version of cause of death data and are subject to further revision by the ABS.
Leading causes of death are based on underlying causes of death and classified using an AIHW-modified version of Becker et al. 2006. International Statistical Classification of Diseases and Related Health Problems, 10th revision (ICD-10) codes are presented in parentheses.
Prostate cancer only affects males and is the 6th leading cause of death for males. Between 1984–1988 and 2009–2013, 5-year relative survival from prostate cancer improved from 58% to 95% [9].
“Men’s health, our way. Let’s own it!” – is a powerful conference theme because it’s a strong foundation for better health.
Owning our health and wellbeing links closely with the Prime Minister’s pledge to do things “with” Aboriginal people, not “to” them – because both commitments empower local community solutions, and personal choices.
This is about walking and working together, because Indigenous health is everybody’s business.
The burden of disease in many of our communities is significant but it is not intractable – we’re here today because we know and believe this.”
The Hon. Ken Wyatt MP Minister for Indigenous Health, Ken Wyatt AM, MP spoke at the NACCHO Ochre Day Men’s Health Conference on 4 October 2017
Good morning everyone.
Before I begin I want to acknowledge the traditional owners of the land on which we meet, the Larrakia people, and pay my respects to Elders past and present.
I also acknowledge all Aboriginal and Torres Strait Islander people here this morning.
I also acknowledge:
John Patterson, [CEO, Aboriginal Medical Services Northern Territory]
June Oscar, [Aboriginal and Torres Strait Islander Social Justice Commissioner]
Dr Mark Wenitong, [Member, Implementation Plan Advisory Group]
“Men’s health, our way. Let’s own it!” – is a powerful conference theme because it’s a strong foundation for better health.
We know that when people are empowered to take control of their own wellbeing, and take that responsibility seriously, we are on track for an improved future.
I’d like to begin by sharing a very sad story, from my own family.
Eight years ago, my nephew, Jason Bartlett was a much-loved musician. He’d made it to the Top 24 on TV’s Australian Idol and was recording albums and performing concerts with the popular Bartlett Brothers band.
But as his career went on, he found he struggled with his weight more and more and his health deteriorated significantly.
Earlier this year, he confided that he wished he had sought help much earlier and that he had listened to the medical professionals who tried to help him along the way.
Sadly, he passed away in June, aged just 35, after a battle with chronic kidney, diabetes and heart conditions.
His close family and friends are now working on a media project to fulfil his dying wishes – to get the word out to indigenous men in particular, to take their health seriously – to own it.
One of Jason’s killers was kidney failure, the same devastating condition that claimed the life of beloved musician, Dr G Yunipingu.
I would like to tell you now that turning around the tragedy of this disease is one of my top priorities.
Our men suffer kidney health problems at five times the rate of non-indigenous men and the onset of kidney disease is at a much earlier age in indigenous people. The rates of kidney disease steadily increase from 18 years as compared to 55 years for non-indigenous.
I will say much more about this in the coming months, but I am totally committed to working with communities and health practitioners across our nation to reduce the impact of renal failure and, even more importantly, to prevent it happening in the first place.
This means solutions that help people now, but also grassroots strategies that will help ensure our men, women and families continue reaping the benefits in five, 10 and 20 years – for the rest of their lives.
Owning our health and wellbeing links closely with the Prime Minister’s pledge to do things “with” Aboriginal people, not “to” them – because both commitments empower local community solutions, and personal choices.
This is about walking and working together, because indigenous health is everybody’s business.
The burden of disease in many of our communities is significant but it is not intractable – we’re here today because we know and believe this.
We understand the importance of Aboriginal community controlled health services because they are delivering many of what I like to call “jewels in the crown” of indigenous health improvement.
Recently, I was delighted to join Matthew to announce the expansion of one of the most successful of all programs– Deadly Choices – as it officially linked in with the Australian Kangaroos rugby league team.
Through sport and community activities, Deadly Choices has empowered thousands of people, especially younger men.
In South East Queensland, this has led to nearly 19,000 people having health check-ups each year, more than 1,100 households banning smoking, and active indigenous patient numbers tripling, to over 330,000.
I was also recently in Broken Hill, and saw firsthand some of the Maari Ma Health Corporation’s impressive results:
People in their diabetes program now have blood sugar control significantly better than the national average.
Those with diabetes or heart problems also have much better blood pressure and cholesterol control than the national average.
The number of people having annual health checks is doubling almost every year.
The number of specialist clinics operating that tackle everything from smoking to ear, nose and throat surgery, has jumped from under 100 to nearly 1000 a year.
And Maari Ma has a rock-solid commitment to local decision-making and employment, with Aboriginal people now making up well over half of the staff.
What is so impressive is the comprehensive nature of these programs – looking beyond the traditional notion of “health”, to a more holistic approach encompassing education, lifestyle and employment.
Working with locals and the community, this helps ensure the “social and cultural determinants” of health are increasingly positive.
The Government’s 2017 Health Performance Framework estimates these factors contribute to more than one third of the health gap.
This figure rises to well over half, when combined with risk factors, such as heavy drinking, smoking and poor diet.
So half of the reason why Aboriginal and Torres Strait Islander men are dying too young, falling sick and getting injured lies largely outside the “traditional” health system.
This is a challenge, but understanding this fact is fundamental to us taking the next steps towards Closing the Gap in indigenous health outcomes .
It’s why the next Implementation Plan for the National Aboriginal and Torres Strait Islander Health Plan 2013 – 2023, due next year, will recognise that respect for culture, employment, living conditions, environmental health and education are ALL-IMPORTANT in the overall health of our people.
The Plan will identify opportunities to develop partnerships further – between communities, the health sector and the wide range of State and Commonwealth Government agencies working in Aboriginal and Torres Strait Islander affairs.
Working closely with local communities and tailor-making solutions, while thinking broadly, is the way forward.
In New South Wales, a program called “Driving Change” is helping indigenous people turn the corner on health and wellbeing, by getting their drivers’ licenses.
Already, its enabled an extra 400 people across a dozen communities to get on the road – and start changing their lives, through better self-esteem and improved employment prospects.
It’s recognised as a health program, because licensed driving means being able to hold down a job, which means having more money, better housing, better food on the table, more options for their children – the list goes on – but the bottom line is a far healthier future.
We have to look at how a wide range of government agencies, and the health sector, throw their weight behind Indigenous opportunity, and how we can do better.
We must ask ourselves constantly: How well are we connecting, how many lives are being changed for the better by what we do?
If we don’t know the answer, then business as usual is not an option.
We clearly have much to do to get the broader health system where it needs to be.
I work with a range of Indigenous organisations, like NACCHO, across the country to put Indigenous families and communities at the centre of Indigenous health reform.
I remain deeply grateful and buoyed by every one of you here, who get up each day and go to work to improve people’s health.
I strongly believe that the key to closing the gap is for all of us to ‘opt-in’ – so there is even more Aboriginal and Torres Strait Islander leadership and participation in the health system.
Higher representation at all levels of the health system – as doctors, nurses, allied health professionals, in administration and management, in policy and planning, and research – will support our efforts to close the gap.
But the fact remains, Indigenous men have the poorest health of any group within the Australian population.
We are more reluctant to seek out help when we need it, we’re not good at recognising the early signs of disease and we don’t always think about what we can do right now – like quitting smoking – to prevent disease down the track.
This is reflected in a range of key health indicators so let’s look at the facts as I outline the Australian Government’s Indigenous men’s health agenda.
On average, we are dying more than 10 years younger than our non-Indigenous counterparts, with the majority of deaths occurring in our middle years.
The leading killers include circulatory failure, cancer, injury, diabetes and respiratory disease.
Infant Indigenous boys die at a rate almost double that of non-Indigenous boys.
This is why the Government has invested $94 million in the Better Start to Life initiative to support families.
This initiative will progressively increase the number of New Directions services from 85 to 136 sites and the Australian Nurse-Family Partnership Program from three sites to 13.
In addition, the Indigenous Australians’ Health Programme has allocated $12 million to support the implementation of better, more integrated early childhood services called Connected Beginnings.
A good foundation in health prevention and regular check-ups will help children do better at school which, in turn, gives them more choice in further education and work opportunities down the track.
While I want much work done to improve renal health, among my other top priorities are hearing, eyesight and preventable hospital admissions.
One area where I am also working hard with local communities, especially in the Territory and the Kimberley, is to reduce the wholly unacceptable rate of suicide.
I’ll talk more about mental health shortly, but figures from 2011–15 reveal that 71 per cent of Indigenous suicides were men.
Indigenous males are hospitalised for diagnoses related to alcohol at 4.2 times the rate of non-Indigenous males (July 2013 – June 2015).
Reducing alcohol abuse can result in fewer assaults and less disability and improve the health and wellbeing of the population.
The National Drug Strategy includes the National Aboriginal and Torres Strait Islander Peoples Drug Strategy to focus on this problem.
Importantly, this initiative has been informed by extensive community consultation.
Tobacco smoking is the most preventable cause of illness and early death among Indigenous men, with 45 per cent of males aged over 15 smoking.
The Government’s $116.8 million Tackling Indigenous Smoking program aims to reduce the uptake of smoking, and increase quit rates.
The successful Don’t Make Smokes Your Story campaign speaks directly to Indigenous smokers. There are encouraging signs, with smoking rates steadily declining every year, and I praise the efforts and commitment of the frontline tobacco workers who have contributed to this improvement.
The Australian Government’s health investments cover key areas of disease burden and risk factors across the entire population, but we give close consideration to what impacts, disproportionately, on Aboriginal and Torres Islander men.
For example, the new Council of Australian Governments National Strategic Framework for Chronic Conditions prioritises Aboriginal and Torres Strait Islander health.
The Government will also soon introduce a new National Male Health Initiative – a partnership with Andrology Australia, the Australian Men’s Health Forum, and the Men’s Health Information and Resource Centre.
This new collaboration will identify needs, and develop, disseminate and evaluate health promotion, education and clinical practice activities right across Australia.
Another priority is to increase Indigenous participation in the National Bowel Cancer Screening Program – so next year, a National Indigenous Bowel Screening Pilot will roll out in 50 Indigenous primary health care services.
Instead of receiving the bowel screening kit in the mail, the pilot will ensure general practitioners, nurses and Indigenous health workers directly offer the kits to people and provide follow up support.
The Government also doubled the number of Commonwealth-funded Prostate Cancer Nurses from 14 up to 28, with many of these working in rural and regional Australia.
The Men’s Sheds program is another mainstream program that helps to reduce the social isolation of men.
Priority is given to sheds in disadvantaged areas that focus on the needs of Aboriginal and Torres Strait Islander men, which leads me to the point I made earlier, about mental health.
Community-led solutions are the most effective, and although we need to work together nationally, each community will have its own response that will work best for them.
Funding of $85 million, over three years, aims to improve access to culturally sensitive, integrated mental health services for Aboriginal and Torres Strait Islander people.
These services will be commissioned locally by local Primary Health Networks, and I have made it clear that they must work closely with the Aboriginal Community Controlled Health Service sector to achieve the best possible outcomes.
I will continue to work with you to build on the reforms we have in place and ensure more responsibility for decision making rests as close to the community as possible.
Everything we do should be grounded in consultation and founded on evidence – using information and local input to understand where progress is slow, or results have flatlined.
Where we find that using the same old approaches is not making a real difference to people’s lives, I want to partner with local people and organisations like the ones you work for, to tackle these particular challenges head-on.
Together, we will build a better tomorrow – by helping our men own their future health.
“Aboriginal and Torres Strait Islander men experience a number of additional challenges compared with non-Indigenous youth and have much higher rates of high/very high levels of psychological distress.
The 2017 Aboriginal and Torres Strait Islander Health Performance Framework report paints a disconcerting picture of mental health issues among Aboriginal men, highlighting the need for holistic and culturally appropriate programs to tackle the epidemic,”
John Patterson, Executive Officer, Aboriginal Medical Services Alliance of the NT (AMSANT), said Australia is currently in the grips of a suicide epidemic, which disproportionately affects young Aboriginal men :
Pictured below with the Indigenous Health Minister Ken Wyatt and Conference Facilitator Dr Mick Adams
see John’s full speech part 2 below
“ Ochre Day aims to raise awareness of issues in Aboriginal men’s health, celebrate the work being done by Aboriginal medical services on the ground in our communities, and encourage indigenous males to have their health checked and seek support,”
Addressing gaps in male Aboriginal health is a key step in reaching the seven targets set by the Council on Australian Governments (COAG) to close the gap between Aboriginal and Torres Strait Islander peoples and non-Indigenous Australians,”
Patrick Johnson, Leadership Project Officer, Aboriginal Medical Service Alliance NT said he hoped the two-day policy summit would assist in identifying gaps in male Aboriginal health care and the development and adoption of a national men’s health strategy
NTGPE Senior Cultural Educator Richard Fejo conducted the Welcome to Country.With Onemobdance group linking arms acknowledging their support of eliminating violence against women.
Pictures Normie Gee
Hundreds of Aboriginal and Torres Strait Islander men and health leaders from across Australia will be meeting in Darwin for a two-day policy summit on the 4th and 5th October to raise awareness of the suicide epidemic and a plethora of other issues in Aboriginal male health.
Mental health and suicide prevention will be among the key issues addressed at this year’s Ochre Day Policy Summit, which will hear from a number of prominent policy makers and public health experts.
The 2017 Aboriginal and Torres Strait Islander Health Performance Framework report cites the 2015 Youth Survey which found that 18% of Aboriginal and Torres Strait Islander young people surveyed had high levels of concern about suicide (compared with 11% non-Indigenous), 18% were concerned about discrimination (compared with 10% non-indigenous) and one in five reported bullying and emotional abuse as a concern.
The same survey found that young Indigenous males were more likely to report very low levels of happiness (10%) than Indigenous females (5%) or non-Indigenous youth (1.2%).
“Aboriginal people are six times likely to commit suicide than non-Aboriginal people, with the Kimberley region in Western Australia recording one of the highest suicide rates in the world.
“We are talking about whole generations of young Aboriginal men and women who are born into families where suicide is normalised and where the grief from suicide persists across multiple generations,” said Mr Patterson.
The first Ochre Day was held in Canberra in 2013.
This year’s Ochre Day, will feature a major address from The Hon Ken Wyatt MP, Minister for Aged Care and Indigenous Health, who will present on the five most serious health problems facing Aboriginal men today and what needs to be done to readily address them.
Other presentations at the policy summit include an overview of Aboriginal men’s health, sexual health, intergenerational trauma, family violence, anger management, youth detention, addiction solutions and healing circles.
Mr Johnson said he hoped the two-day policy summit would assist in identifying gaps in male Aboriginal health care and the development and adoption of a national men’s health strategy.
“Addressing gaps in male Aboriginal health is a key step in reaching the seven targets set by the Council on Australian Governments (COAG) to close the gap between Aboriginal and Torres Strait Islander peoples and non-Indigenous Australians,” said Mr Johnson.
“Aboriginal men must have the same access to health care as other Australians and in particular, tailored, culturally appropriate programs must be developed to address mental health, social and emotional well being and suicide prevention.
“We need to invest more in grassroots programs delivered by Aboriginal people, for Aboriginal people, if we want to have a fighting chance to turn around the harrowing statistics which have seen too many of our sons, fathers and uncles die young.
“We have made great strides already, however there is much more work to be done before we reach the point where a new generation of young Aboriginal men emerges where issues such as suicide are no longer entrenched and normalised,” said Mr Johnson.
National Ochre Day Opening Remarks – AMSANT CEO, John Paterson
Darwin, 4 October 2017
Firstly, I would like to acknowledge we’re meeting today on Larrakia traditional land and thank Richard and Tony for their welcome.
I would also like to welcome participants to this national Ochre Day event, and to acknowledge dignitaries here with us today
This is an important gathering as it is too seldom that we are able to come together as a group of Aboriginal men to work on how we want to address the health challenges that continue to confront Aboriginal men in Australia today.
NACCHO is to be congratulated for developing Ochre Day as a national opportunity for us to do this.
Over the next two days we will explore our theme “Men’s Health, Our Way. Let’s Own It!” The theme reminds us that we do have to take ownership of our health and, just as importantly, provide leadership in telling government what is needed to bring the health of Aboriginal men up to where it should be.
I don’t need to tell any of you that the state of Aboriginal male health is not good. The gap in life expectancy alone remains far too great. Nationally, while life expectancy for Aboriginal men has increased from just over 67.5 years in 2005-07 to 69.1 years in 2011-12, the gap between Aboriginal men and non-Aboriginal men is still too large at 10.6 years. However, if we look at the gap between Aboriginal men in the Territory and national male life expectancy, the gap is 16.4 years!
It’s important, gathering where we are here in Darwin, in the Northern Territory, that we acknowledge just how significantly worse the health of Aboriginal Territorians is than the health of Aboriginal people nationally. For Aboriginal men in the Territory this translates to a life expectancy that is on average 4 years less than for Aboriginal men nationally.
Overall, the mortality rate for Aboriginal Territorians is 50% higher when compared with Indigenous people interstate, and 85% higher than non-Aboriginal Territorians.
And for Aboriginal men in the Territory, we experience a 10-15% higher mortality than our Aboriginal women.
Clearly, there is a long way to go in closing the health gap for Aboriginal men and achieving the standard of health and wellbeing that we would all like to see.
This raises an important issue. Beyond just the statistics, what does health and wellbeing mean for us as Aboriginal men?
The Aboriginal concept of health is not just an absence of illness. It is not just the physical well-being of an individual. It refers also to the social, emotional, spiritual and cultural well-being of the whole Community. It means each individual being able to achieve their full potential as a human being and contributing to the total well-being of their Community. It is a whole of life view and includes the cyclical concept of life-death-life.
So, when we talk about “Our way” and about “Let’s own it”, we’re talking as much about our spiritual and psychological health as we are about our physical health.
For us to achieve our full potential as human beings, we must deal with the legacies of our own lives, and also the lives of our fathers and grandfathers and the generations before them. Some of these are heavy legacies.
Aboriginal men have been wounded by the impacts since colonisation which devalued our cultures, dispossessed and dislocated our families and communities and introduced diseases.
Our elders lost their roles with authority and status, and young males lost their role models.
This has diminished the status, self-esteem and sense of purpose of Aboriginal males and contributed to alcohol abuse, self-harm and violence.
It has caused trauma to successive generations, and that trauma continues.
The impacts of trauma will be discussed later this morning, but I wanted to raise here one source of impact from recent years that has impacted heavily on Aboriginal men in the Territory – the NT Intervention.
This top-down, punitive attack on Aboriginal communities in the NT, maliciously targeted Aboriginal men as child abusers, as corrupt and devoid of basic humanity. It was used to strip us of our dignity and as an excuse to subject us to coercive controls on our lives and on our communities.
The extent of the damage to communities caused by the Intervention will probably never be fully known, but I do know that every Aboriginal Territorian man in this room will have felt its impact in some way.
As a policy, its failure is perhaps most evident in the billions of dollars spent with so little to show in terms of positive outcomes.
And only in the last couple of years has the tide begun to turn, with governments at both Commonwealth and Territory levels starting to recognise the need to positively re-engage and to work with us. To bring us back into engagement over policy design and decision-making, and hopefully increasingly into delivering our own services to our communities. As we are doing successfully in the Aboriginal community controlled health sector.
Such rethinking by government I’m sure is also mindful of the ongoing failure of recent policy approaches and funding to improve the structural and social factors or the social determinants of health, that underlie poor health outcomes. Housing, education, employment, access to services, unacceptable rates of imprisonment and children in care.
The inescapable fact, as evidenced by the painfully slow progress on Closing the Gap targets, is that a fundamental change in approach must occur. Such change must start with improving support for the positive social determinant enablers: control, empowerment, and the strength of culture and connection with land.
Being healthy builds on strengths and Aboriginal men have many strengths. We are fathers, husbands, brothers and our communities rely on us. We are resilient and we have the opportunity to use that resilience both for the current generation and for young males and the next generations.
It is important that Aboriginal males continue to be active participants in defining our social roles, both within our own communities and in the broader Australian society.
We need to take back responsibility for traditional practices, parenting and spirituality, as these will contribute to better health.
We have to find ways to contribute our knowledge, skills and authority to initiatives and interventions that concern our health.
Events like Ochre Day and putting together Aboriginal Men’s health strategies are one way we can do this.
We will have a significant focus during this Ochre Day conference on issues related to trauma, social and emotional wellbeing and suicide. These are not easy issues to talk about but they are so important to men’s health. Suicide continues to be a major and avoidable cause of death for Aboriginal men and an issue that we must talk about. Aboriginal and Torres Strait Islander men between 25 and 29 have the highest suicide rates in the entire world, according to a study of youth health released last year.
If anyone is feeling upset or distressed about these conversations, staff from Danila Dilba Health Service are here and you can talk to them about any support you might need. Joseph Knuth is the best person to approach if you need any support at all.
The Conference though will be positive, we will be working on solutions and ideas for the future. We will be taking control!
Today we will hear about men’s health issues and about some of the services that have been developed here in the Northern Territory to bring men into health services in appropriate ways and to empower men to take control of their own health.
We will hear from the top Aboriginal and non-Aboriginal experts in men’s health.
Tomorrow, we will take what we have learned today and start to work towards the future, towards our own solutions and strategies.
We are fortunate to have Dr Mick Adams with us to facilitate discussions towards developing a national Aboriginal men’s health strategy.
This has been a long-held aim in Aboriginal health and has met with considerable difficulty in getting government buy in and commitment.
But we won’t give up, a national strategy is a necessary first step in closing the health gap and building on the strengths of Aboriginal men, families and communities.
I look forward to Dr Adams’ advice and direction on how we might move forward to achieve this.
There will be a lot of opportunity to work together and for all voices to be heard so I encourage everyone to take these opportunities and speak up over the next two days.
Use your Human Resources management experience to enhance remote community health & wellbeing! Great work/life balance & benefits!
About the Organisation
Sunrise Health Service Aboriginal Corporation’s (Sunrise) (ICN 4170) is an Aboriginal Community Controlled Organisation (an ACCHO). An ACCHO is a primary health care service initiated and operated by the local Aboriginal community to deliver holistic, comprehensive, and culturally appropriate health care to the community which controls it, through a locally elected Board of Management. Sunrise’s focus is to improve the health and wellbeing of the people in the Arnhem Land region east of Katherine in the Northern Territory. Sunrise operates nine clinics located across Arnhem Land.
Sunrise works closely with various organisations in the Northern Territory, including the Northern Territory Primary Health Network (NT PHN). NT PHN provides support services to health professionals and organisations across the Northern Territory including support and assistance to health professionals relocating to the NT.
Sunrise has achieved ISO 9001 certification, and accreditation by Australian General Practice Accreditation Limited.
About the Opportunity
Sunrise Health Service Aboriginal Corporation (ICN 4170) now has a full-time opportunity for an experienced HR Manager to join their dedicated, multidisciplinary team.
This is an influential ‘hands-on’ role that offers you the opportunity to advance your career as part of a respected organisation.
The position offers an attractive remuneration package $115,858 – $129,430 (negotiable with skills and experience), plus statutory superannuation. In addition, you will receive a range of benefits including:
6 weeks leave per year
2 weeks study leave
Salary sacrificing options
Additionally, working at Sunrise Health Service and living in the Katherine region has lifestyle benefits that are unique to the Northern Territory. With Australia’s most stunning landscapes on your doorstep and an incredible outdoor lifestyle on offer, the Northern Territory is the place to be to make the most of life’s adventures.
Interviews will be taking place immediately – Apply Now!
Location: Alice Springs | Job ID: 3672893 | Closing Date: 31 Dec 2017
10-12. AHMRC full-time Vacancies
10. Chief Executive Officer
Aboriginal Health and Medical Research Council of NSW is currently seeking a motivated and highly experienced CEO to lead AH&MRC to a new level of sustainable growth and success.
This is an Identified Position.
Applications close: Monday, 9 October 2017.
To receive a copy of the Recruitment Information Package for more information and the selection criteria, please contact HR via email or telephone. The selection criteria must be addressed for your application to be considered.
11.Research, Training and Workforce Development Manager
Located at Little Bay at the Aboriginal Health College.
For a position description please email hr@ahmrc.org.au
Applications close: Monday, 23 October 2017.
12.Government Policy and Partnership Manager
Located at our main office in Surry Hills
This is an Identified Position.
For a position description please email hr@ahmrc.org.au
Applications close: Monday, 23 October 2017.
For a confidential conversation please contact Human Resources on (02) 9212 4777 or email gagic@ahmrc.org.au
Pursuant to Section 14(d) of the Anti-Discrimination Act 1977 (NSW), Australian Aboriginality is a genuine occupational qualification for this position and is identified as an essential pre-requisite for appointment to the role of Chief Executive Officer, under AH&MRC Constitutional Rules.
Aboriginal and/or Torres Strait Islander people are strongly encouraged to apply.
All applicants must address the selection criteria to be considered for the above positions
13-23 ; Durri Aboriginal Corporation Medical Service (Durri ACMS)
The Durri Aboriginal Corporation Medical Service (Durri ACMS) was established in 1976. The name Durri means “to grow in good health” and was bestowed upon the organisation by members of the local Aboriginal community.
Located in Kempsey, approximately half way between the cities of Brisbane and Sydney. Durri is on the traditional land of the Dunghutti peo
Durri’s vision is to achieve and maintain better health and wellbeing outcomes for our Aboriginal people and communities.
Durri aims to be an employer of choice in Aboriginal health, supporting a skilled and flexible workforce.
Durri is a great place to work – a family friendly and culturally sensitive work environment that values people.
If you have a passion for indigenous health and are committed to closing the gap, then why not join us?
WALGETT & BREWARRINA District & COMMUNITY, Nthn-NSW
ESTABLISHED, SUCCESSFUL & HIGHLY RESPECTED ACCHS TEAM
Download this Job info
OUR ORGANISATION
The WALGETT Aboriginal Medical Service (‘WAMS’) and the BREWARRINA Aboriginal Health Service Limited (‘BAHSL’) are highly respected and established Aboriginal Community Controlled Health Organisations, fully committed to providing accessible, practical, culturally appropriate and confidential Health services in Walgett, Brewarrina and surrounding communities.THE OPPORTUNITY
We are looking for a motivated, experienced and suitably qualified individual to join our senior management team, and fulfil the key role of HUMAN RESOURCE MANAGER.
Reporting directly to the Chief Executive Officer, the HR Manager oversees and facilitates all Human Resource and Employee Relations activities of the organisation, including providing timely, practical advice and ongoing strategic support on all employee initiatives, programs and/or workplace issues.
As a key member of the Senior Management Team, the HR Manager is responsible for ensuring HR practices align with strategic business plans for the organisation. This opportunity represents a rewarding and fulfilling opportunity to join our established team, already highly regarded for making a real difference in our local communities. Highly competitive remuneration (including salary packaging), plus local Accommodation options are also available.
Gidgee Healing is an Aboriginal Community Controlled Health Service dedicated to making a long-term positive impact on the health and well being of Aboriginal and Torres Strait Islander families.
Based in Mt Isa, we provide a broad range of high-quality Primary Health Care services across the Mt Isa, North West and Lower Gulf regions of Queensland.
Our multi-disciplinary team comprises GPs, Registered Nurses, Aboriginal Health Practitioners/Workers, Midwives, visiting Allied Health professionals and Medical Specialists and a range of other Workers that support our holistic approach to service delivery.
Gidgee Healing values community participation when planning and delivering our services, to ensure we are meeting the health and wellbeing needs of local Aboriginal and Torres Strait Islander people.
With a service footprint of approximately 640,000 km2, Gidgee Healing has the largest land area of all Aboriginal Community Controlled Health Services in Queensland.
Salary Range: Pending qualification and years of experience (base salary $71,895 – $85,800), 5 weeks annual leave (17.5% leave loading), professional development allowance, superannuation, salary packaging available
Reports to: Allied Health Team Leader – Senior
Positions supervised: Nil
Location: Mount Isa – will require some travel to other remote communities across the North West and Lower Gulf of Carpentaria region
Salary Range: Pending qualification and years of experience (base salary $71,895 – $85,800), 5 weeks annual leave (17.5% leave loading), professional development allowance, superannuation, salary packaging available
Reports to: Allied Health Team Leader – Senior
Positions supervised: Assist with supervision AHA
Location: Mount Isa – will require some travel to other remote communities across the North West and Lower Gulf of Carpentaria region
Salary Range: Pending qualification and years of experience (base salary $71,895 – $85,800), 5 weeks annual leave (17.5% leave loading), professional development allowance, superannuation, salary packaging available
Reports to: Allied Health Team Leader – Senior
Positions supervised: Assist with supervision AHA
Location: Mount Isa – will require some travel to other remote communities across the North West and Lower Gulf of Carpentaria region
Salary Range: Pending qualification and years of experience (base salary $79,000 – $95,000), 5 weeks annual leave (17.5% leave loading), professional development allowance, superannuation, salary packaging available
Reports to: Allied Health Team Leader – Senior
Positions supervised: Nil
Location: Mount Isa – will require some travel to other remote communities across the North West and Lower Gulf of Carpentaria region
29. Miwatj Health NT Senior Social and Emotional Well Being Therapeutic Clinician
Miwatj Health Aboriginal Corporation is the regional Aboriginal Community Controlled Health Service in East Arnhem Land, providing comprehensive primary health care services for over 6,000 Indigenous residents of North East Arnhem and public health services for close to 10,000 people across the region.
Miwatj Health aims to improve access to integrated, culturally responsive and safe mental health and drug and alcohol services that holistically meet the social and emotional well being and mental health needs of the population in the East Arnhem region. We are seeking enthusiastic, dedicated and an appropriately qualified senior therapeutic clinician to fill a role within our organisation.
Our Values
Compassion care and respect for our clients and staff and pride in the results of our work.
Cultural integrity and safety, while recognising cultural and individual differences.
Driven by evidence-based practice.
Accountability and transparency.
Continual capacity building of our organisation and community.
In this role you will be responsible for working collaboratively with members of the Social and Emotional Well Being (SEWB) team, and the Manager, Mental Health to contribute to the development and delivery of the Miwatj SEWB model.
Key Responsibilities include;
Demonstrated experience in working in Aboriginal Community Controlled Health Organisations or environments and fully embrace the concept of Aboriginal Community Control
Experience in delivering (culturally adapted) Focused Psychological Strategies to Aboriginal and Torres Strait Islander people
Deliver culturally adapted evidence based therapeutic interventions that value and build upon traditional indigenous knowledge
Contribute to a coordinated approach for the prevention, assessment, early intervention, referral and shared care arrangements for common mental and behavioral disorders, including alcohol and drug use disorders
Develop and articulate a Miwatj SEWB Model that includes the promotion of strong SEWB, screening, self-referral and early intervention for common mental health disorders (including alcohol and drug use disorders) as part of comprehensive primary health care. This includes the development of mental health care plans, clinical pathways, case management, and clear referral pathways and processes
Develop clinical governance structures and processes to support the delivery of culturally-adapted evidence-based therapeutic interventions to address common mental health disorders, including alcohol and drug use disorders, as part of comprehensive primary health care
Ensure Therapeutic Work complements and works in an integrated way with the existing medical and social/cultural support streams of care
Effectively manage a team of two clinicians to deliver, articulate and promote the SEWB Miwatj Model
To apply for this role you must be either a registered Clinical Psychologist, Registered Psychologist, Mental Health experienced Social Worker, or Mental Health experienced Occupational Therapist and be eligible to work in Australia.
For further details please refer to the Job Description.
This is a full time position with benefits and an attractive salary commensurate with experience. The position is Darwin based and will involve regular travel throughout the Miwatj region (locally based and subsidised accommodation may be negotiated).
Applications close 11 October 2017.
Aboriginal and Torres Strait Islanders are encouraged to apply.
30. Wuchopperen Health Service Cairns : CHIEF EXECUTIVE OFFICER
• Focus on Aboriginal and Torres Strait Islander Health
• Primary and Allied Health Care – Established Services
• Aboriginal Community Controlled Organisation
• Cairns and Outreach Locations
Wuchopperen Health Service Limited is a community controlled organisation delivering holistic primary and allied health care for Aboriginal and Torres Strait Islander people in Cairns and surrounding districts. Wuchopperen Health Service’s vision of improving quality of life for Aboriginal and Torres Strait Islander Peoples underlines our commitment to providing high quality, safe and coordinated care for our people.
Wuchopperen is seeking a motivated and appropriately experienced CEO to deliver inspirational leadership and continue to drive our strategic aims to fully develop our organisations potential, enhance our capability and continue to expand the key role we already play within our community, now and into the future.
Reporting directly to the Board of Directors, the successful applicant will oversee an established organisational structure comprising of Clinic, Allied Health, Community and Mental Health Services, a Child and Family Centre along with Corporate Support.
The CEO will provide clear direction in the effective coordination of our various health services and programs, and funding related activity. In addition, the CEO will be responsible for facilitating corporate governance responsibilities and working closely with and alongside the Board, and providing oversight of Wuchopperen’s ongoing strict adherence to relevant Accreditation and Funding compliance standards.
This role presents an outstanding opportunity for a suitably inspired and credentialed Indigenous professional, to oversee the ongoing success and continual improvement of our organisation in accepting responsibility for the following key areas: Board Governance, Compliance and Coordination
• Leadership and Management of the Executive Team
• Strategic Management and Planning within a Competitive Health Market
• Budget, Finance, Risk Assessment and Funding
• Representation and Advocacy of Wuchopperen
• Local, Regional and National Stakeholder Engagement
• Business Development and Revenue Enhancement
Please submit your application, including a cover letter and resume, to Jenny Hall at jenny@mjsp.com.au.
31-36 : Wurli-Wurlinjang Health NT 6 positions
If you are considering applying for a position with us, we encourage you in the first instance to review the position profile of the vacancy you are interested in. This will assist you in understanding the role you are interested in and will provide details in relation to the position responsibilities and other criteria applicants should consider addressing in their application.
All applications must contain the following as a minimum:
completed employment application form
current resume or curriculum vitae (CV)
a cover letter which provides a clear and concise overview of your ability to meet the requirements of the role.
a minimum of two referees (names, positions and telephone contact number) preferably one current and one past supervisor
Note: Applications who are successful must have the ability to satisfactorily complete a Criminal History Check and obtain a Working with Children Card.
Applications may be forwarded using our online Employment Application Form OR by emailing the Human Resources team at hr@nullwurli.org.au
33.Strong Indigenous Families. Positions include: Counsellors/ Therapists, Case Managers & Community Engagement Support Officers (FDV)
34.Mental Health Professionals
35.Registered Aboriginal Health Practitioner
36.General Practitioner
37 – 47 JOBS AT IUIH Brisbane
IUIH and its members are constantly looking for healthcare workers, GP’s, allied health professionals, medical and health related students to fill short or long term vacancies within their growing operations.Current job opportunities are listed below:
About the Position
AMSANT is seeking a competent and motivated Accountant for our finance team with good interpersonal and organisational skills and a passion for contributing to improvements in Aboriginal health in the NT. The successful candidate will preferably hold a degree in Accounting with a minimum of two years’ experience. Duties will consist of processing the AMSANT fortnightly payroll for 45 staff, processing monthly and annual accruals, reconciling and lodgement of ATO requirements, maintaining asset register, managing AMSANT funding compliance register and other finance duties and ad hoc reporting. Experience with Payroll and MYOB is highly desirable.
Contract Type & Salary
This is a full time role with salary between $80,559 and $85,465 based on the successful applicant’s experience and qualifications. Generous salary packaging is also available.
Location
Darwin
How to apply Please download the Job Description and Selection Criteria above.
Your application should address the selection criteria and include a CV, cover letter and two referee’s details. Email applications to hr@amsant.org.au
Application closing date
15th October 2017
For further information about the role Contact Paul Stephson or Human Resources on 08 8944 6666/ hr@amsant.org.au
We strongly encourage applications from Aboriginal and Torres Strait Islander peoples for all positions that become available at AMSANT.
This report expands on the key findings from the 2016 National Drug Strategy Household Survey (NDSHS) that were released on 1 June 2017.
It presents more detailed analysis including comparisons between states and territories and for population groups. Unless otherwise specified, the results presented in this report are for those aged 14 or older.
Indigenous Australians
As Indigenous Australians constitute only 2.4 per cent of the 2016 NDSHS (unweighted) sample (or 568 respondents), the results must be interpreted with caution, particularly those for illicit drug use.
Smoking
In 2016, the daily smoking rate among Indigenous Australians was considerably higher than non-Indigenous people but has declined since 2010 and 2013 (decreased from 35% in 2010 to 32% in 2013 and to 27% in 2016) (Figure 8.7). The NDSHS was not designed to detect small differences among the Indigenous population, so even though the smoking rate declined between 2013 and 2016, it was not significant.
The Australian Aboriginal and Torres Strait Islander Health Survey (AATSIHS) and the National Aboriginal and Torres Strait Islander Social Survey (NATSISS) were specifically designed to represent Indigenous Australians (see Box 8.1 for further information).
After adjusting for differences in age structures, Indigenous people were 2.3 times as likely to smoke daily as non-Indigenous people in 2016 (Table 8.7).
Overall, Indigenous Australians were more likely to abstain from drinking alcohol than non-Indigenous Australians (31% compared with 23%, respectively) and this has been increasing since 2010 (was 25%) (Figure 8.8).
Among those who did drink, a higher proportion of Indigenous Australians drank at risky levels, and placed themselves at harm of an alcoholrelated injury from single drinking occasion, at least monthly (35% compared with 25% for non-Indigenous).
The (rate ratio) gap in drinking rates was even greater when looking at the consumption of 11 or more standard drinks at least monthly. Indigenous Australians were 2.8 times as likely as non-Indigenous Australians to drink 11 or more standard drinks monthly or more often (18.8% compared with 6.8%).
About 1 in 5 (20%) Indigenous Australian exceeded the lifetime risk guidelines in 2016; a slight but non-significant decline from 23% in 2013, and significantly lower than the 32% in 2010. The proportion of non-Indigenous Australians exceeding the lifetime risk guidelines in 2016 was 17.0% and significantly declined from 18.1% in 2013.
Illicit drugs
Other than ecstasy and cocaine, Indigenous Australians aged 14 or older used illicit drugs at a higher rate than the general population (Table 8.6). In 2016, Indigenous Australians were: 1.8 times as likely to use any illicit drug in the last 12 months; 1.9 times as likely to use cannabis; 2.2 times as likely to use meth/amphetamines; and 2.3 times as likely to misuse pharmaceuticals as non-Indigenous people. These differences were still apparent even after adjusting for differences in age structure (Table 8.7). There were no significant changes in illicit use of drugs among Indigenous Australians between 2013 and 2016.
1 in 8 Australians smoke daily and 6 in 10 have never smoked
Smoking rates have been on a long-term downward trend since 1991, but the daily smoking rate did not significantly decline over the most recent 3 year period (was 12.8% in 2013 and 12.2% in 2016).
Among current smokers, 3 in 10 (28.5%) tried to quit but did not succeed and about 1 in 3 (31%) do not intend to quit.
People living in the lowest socioeconomic areas are more likely to smoke than people living in the highest socioeconomic area but people in the lowest socioeconomic area were the only group to report a significant decline in daily smoking between 2013 and 2016 (from 19.9% to 17.7%).
8 in 10 Australians had consumed at least 1 glass of alcohol in the last 12 months
The proportion exceeding the lifetime risk guidelines declined between 2013 and 2016 (from 18.2% to 17.1%); however, the proportion exceeding the single occasion risk guidelines once a month or more remained unchanged at about 1 in 4.
Among recent drinkers: 1 in 4 (24%) had been a victim of an alcohol-related incident in 2016; about 1 in 6 (17.4%) put themselves or others at risk of harm while under the influence of alcohol in the last 12 months; and about 1 in 10 (9%) had injured themselves or someone else because of their drinking in their lifetime.
Half of recent drinkers had undertaken at least some alcohol moderation behaviour. The main reason chosen was for health reasons.
A greater proportion of people living in Remote or very remote areas abstained from alcohol in 2016 than in 2013 (26% compared with 17.5%) and a lower proportion exceeded the lifetime risk guidelines (26% compared with 35%).
About 1 in 8 Australians had used at least 1 illegal substance in the last 12 months and 1 in 20 had misused a pharmaceutical drug
In 2016, the most commonly used illegal drugs that were used at least once in the past 12 months were cannabis (10.4%), followed by cocaine (2.5%), ecstasy (2.2%) and meth/amphetamines (1.4%).
However, ecstasy and cocaine were used relatively infrequently and when examining the share of Australians using an illegal drug weekly or more often in 2016, meth/amphetamines (which includes ‘ice’) was the second most commonly used illegal drug after cannabis.
Most meth/amphetamine users used ‘ice’ as their main form, increasing from 22% of recent meth/amphetamine users in 2010 to 57% in 2016.
Certain groups disproportionately experience drug-related risks
Use of illicit drugs in the last 12 months was far more common among people who identified as being homosexual or bisexual; ecstasy and meth/amphetamines use in this group was 5.8 times as high as heterosexual people.
People who live in Remote and very remote areas, unemployed people and Indigenous Australians continue to be more likely to smoke daily and use illicit drugs than other population groups.
The proportion of people experiencing high or very high levels of psychological distress increased among recent illicit drug users between 2013 and 2016—from 17.5% to 22% but also increased from 8.6% to 9.7% over the same period for the non-illicit drug using population (those who had not used an illicit drug in the past 12 months).
Daily smoking, risky alcohol consumption and recent illicit drug use was lowest in the Australian Capital Territory and highest in the Northern Territory.
The majority of Australians support policies aimed at reducing the acceptance and use of drugs, and the harms resulting from drug use
There was generally greater support for education and treatment and lower support for law enforcement measures.
‘In 2016, 42% of meth/amphetamine users had a mental illness, up from 29% in 2013, while the rate of mental illness among ecstasy users also rose from 18% to 27%,’ said AIHW spokesperson, Matthew James. ‘Drug use is a complex issue, and it’s difficult to determine to what degree drug use causes mental health problems, and to what degree mental health problems give rise to drug use.’
About 1 in 20 Australians reported misusing pharmaceuticals, with 75% of recent painkiller users reporting misusing an ‘over the counter’ codeine product in the past 12 months. The AIHW will be publishing more detailed data on pharmaceutical misuse later in 2017.
In addition to illicit drugs, the report also provides insights into Australians’ use of alcohol and tobacco, and notes some improvements in risky behaviour (such as driving while under the influence of alcohol), as well as improved smoking rates among people living in lower socioeconomic areas.
Source: Australian Institute of Health and Welfare
Part 3 Mental illness rising among meth/amphetamine and ecstasy users
Mental illnesses are becoming more common among meth/amphetamine and ecstasy users, according to a report released today by the Australian Institute of Health and Welfare (AIHW).
The report, National Drug Strategy Household Survey: detailed findings 2016, builds on preliminary results released in June, and gives further insight into Australians’ use of, and attitudes to, drugs and alcohol in 2016.
The report shows that among people who had recently (in the last 12 months) used an illicit drug, about 27% had been diagnosed or treated for a mental illness—an increase from 21% in 2013. Rates of mental illness were particularly high—and saw the most significant increases—for meth/amphetamine and ecstasy users.
‘In 2016, 42% of meth/amphetamine users had a mental illness, up from 29% in 2013, while the rate of mental illness among ecstasy users also rose from 18% to 27%,’ said AIHW spokesperson Matthew James.
‘Drug use is a complex issue, and it’s difficult to determine to what degree drug use causes mental health problems, and to what degree mental health problems give rise to drug use’.
Similarly, the report also reveals a complex relationship between employment status and drug use.
‘For example, people who were unemployed were about 3 times as likely to have recently used meth/amphetamines as employed people, and about 2 times as likely to use cannabis or smoke tobacco daily. On the other hand, employed people were more likely to use cocaine than those who were unemployed,’ Mr James said.
Today’s report also shows higher rates of drug use among people who identify as gay, lesbian or bisexual, with the largest differences seen in the use of ecstasy and meth/amphetamines.
‘Homosexual and bisexual people were almost 6 times as likely as heterosexual people to use each of these drugs, and were also about 4 times as likely to use cocaine as heterosexual people, and 3 times more likely to use cannabis or misuse pharmaceutical drugs.’ Mr James said.
Overall, about 1 in 20 Australians reported misusing pharmaceuticals, with 75% of recent painkiller users reporting misusing an ‘over the counter’ codeine product in the past 12 months. The AIHW will be publishing comprehensive data on pharmaceutical misuse later in 2017.
‘Our report also shows that more Australians are in favour of the use of cannabis in clinical trials to treat medical conditions—87% now support its use, up from 75% in 2013. We also found that 85% of people now support legislative changes to permit its use for medical purposes in general, up from 69% in 2013,’ Mr James said.
In addition to illicit drugs, today’s report also provides insights into Australians’ use of alcohol and tobacco, and notes some improvements in risky behaviour (such as driving while under the influence of alcohol), as well as improved smoking rates among people living in lower socioeconomic areas.
The report also contains data for each state and territory in Australia, and shows differences in drug use between the jurisdictions. For example, recent use of meth/amphetamine was highest in Western Australia, but the use of cocaine was highest in New South Wales.
4- 5 October Aboriginal Male Health Ochre Day Darwin NT
2017 Ochre Day follow on Twitter #OchreDay2017
Where: Darwin Starts tomorrow : 4th & 5th October 2017
This year NACCHO is pleased to announce the annual NACCHO Ochre Day will be held in Darwin
Beginning in 2013, Ochre Day is an important NACCHO Aboriginal male health initiative. Aboriginal males have arguably the worst health outcomes of any population group in Australia.
NACCHO has long recognised the importance of addressing Aboriginal male health as part of Close the Gap by 2030.
9- 10 October Indigenous Affairs and Public Administration Conference : Can’t we do better?
This year marks 50 years since the 1967 referendum resulted in the Commonwealth gaining national responsibilities for the administration of Indigenous affairs. This is a shared responsibility with state and territory administrations.
ANZSOG and the Department of the Prime Minister and Cabinet are providing travel support and waiving conference fees for Aboriginal and Torres Strait Islander community leaders and public servants attending the conference from remote locations.
In partnership, the Department of the Prime Minister and Cabinet (DPMC), the University of Sydney, and the Australia and New Zealand School of Government (ANZSOG) are holding an international conference that questions the impact of the past 50 years of public administration and raise issues for the next 50 years in this important nation building area.
DPMC is seeking to build and foster a public canon of knowledge to open the history of Indigenous policy and administrative practice to greater scrutiny and discussion.
The Indigenous Affairs and Public Administration Conference will be attended by Aboriginal and Torres Strait Islander representatives, other Indigenous peoples, public servants from state and federal governments, and the academic community.
The conference will feature a range of guest presenters, including Australia’s Chris Sarra, Andrea Mason and Martin Nakata, New Zealand’s Arapata Hakiwai and Geraint Martin, as well as other international speakers.
The deliberations and discussions of the conference will feed into a final report that will be used to guide Federal government policy formation at a series of roundtables in late 2017 and early 2018.
11-12 October 3rd Annual Ngar-wu Wanyarra Aboriginal Health Conference
3rd Annual Ngar-wu Wanyarra Aboriginal Health Conference
The Ngar-wu Wanyarra Aboriginal Health conference is an opportunity for sharing information and connecting people that are committed to reforming the practice and research of Aboriginal health and celebrates Aboriginal knowledge systems and strength based approaches to improving the health outcomes of Aboriginal communities.
The conference will include evidence based approaches, Aboriginal methods and models of practice, Aboriginal perspectives and contribution to health or community led solutions, underpinned by cultural theories to Aboriginal health and wellbeing.
In 2016 the Ngar-wu Wanyarra Aboriginal Health conference attracted over 130 delegates from across the community and state.
Please register online by midday Thursday 5th October, 2017.
18 -20 October 35th Annual CRANAplus Conference Broome
We are pleased to announce the 35th Annual CRANAplus Conference will be held at Cable Beach Club Resort and Spa in Broome, Western Australia, from 18 to 20 October 2017.
THE FUTURE OF REMOTE HEALTH AND THE INFLUENCE OF TECHNOLOGY
Since the organisation’s inception in 1982 this event has served to create an opportunity for likeminded remote and isolated health individuals who can network, connect and share.
It serves as both a professional and social resource for the Remote and Isolated Health Workforce of Australia.
We aim to offer an environment that will foster new ideas, promote collegiate relationships, provide opportunities for professional development and celebrate remote health practice.
The First 1000 Days Australia Summit is a three-day event that will bring together Aboriginal and Torres Strait Islander Elders, researchers, community members, front- line workers and policy makers involved in areas relevant to the work of First 1000 Days Australia. Lectures, panel discussions and workshops will address topics such as caring and parenting, infant and child development, family strengthening, implementation and translation, as well as a number of other areas.
The theme for the Summit is ‘Celebrating our leadership, strengthening our families’. We invite interested presenters to submit abstracts for oral presentations, workshops and posters that align with the aims, principles and research areas of First 1000 Days Australia, and of First 1,000 Days international.
Australia’s most influential health leaders will discuss critical health policy issues in a key Presidents’ Breakfast forum at the Rural Medicine Australia 2017 conference, to be held in Melbourne in October.Dr Ewen McPhee, President of the Rural Doctors Association of Australia (RDAA), will host the forum and will be joined on the panel by Associate Professor Ruth Stewart, President of the Australian College of Rural and Remote Medicine (ACRRM); Dr Bastian Seidel, President of the Royal Australian College of General Practitioners (RACGP); and Dr Tony Bartone, Vice President of the Australian Medical Association (AMA).
26-27 October Diabetes and cardiovascular research, stroke and maternal and child health issues.
‘Translation at the Centre’ An educational symposium
Alice Springs Convention Centre, Alice Springs
This year the Symposium will look at research translation as well as the latest on diabetes and cardiovascular research, stroke and maternal and child health issues. The event will be run over a day and a half.
The Educational Symposium will feature a combination of relevant plenary presentations from renowned scientists and clinicians plus practical workshops.
Registration is free but essential.
Please contact the symposium coordinator on 1300 728 900 (Monday-Friday, 9am-5pm) or via email at events@baker.edu.au
31 October –2 NovNACCHO AGM Members Meeting Canberra
We welcome you to attend the 2017 NACCHO Annual Members’ Conference.
Download the 12 page PDF Draft Program as at 26 September
The NACCHO Members’ Conference and AGM provides a forum for the Aboriginal community controlled health services workforce, bureaucrats, educators, suppliers and consumers to:
Present on innovative local economic development solutions to issues that can be applied to address similar issues nationally and across disciplines
Have input and influence from the ‘grassroots’ into national and state health policy and service delivery
Demonstrate leadership in workforce and service delivery innovation
Promote continuing education and professional development activities essential to the Aboriginal community controlled health services in urban, rural and remote Australia
Promote Aboriginal health research by professionals who practice in these areas and the presentation of research findings
Develop supportive networks
Promote good health and well-being through the delivery of health services to and by Indigenous and non-Indigenous people throughout Australia.
Where :Hyatt Hotel Canberra
Dates :Members’ Conference: 31 October – 1 November 2017 Annual General Meeting: 2 November 2017
National Aboriginal and Torres Strait Islander Health Workers Association (NATSIHWA)
Join the National Aboriginal and Torres Strait Islander Health Workers Association (NATSIHWA) for a one day CPD networking workshop focussed on current workforce development opportunities.
Upskill and strengthen your skill level in a specialised area and find out what is happening through program development, education and funding opportunities.
Hear from organisations such as: PHN Primary Heath Network, CranaPlus, Autism QLD, Rheumatic Heart, PEPA Program of Experience in the Palliative Approach, Diabetes Australia, IBA Indigenous Business Australia, HESTA Superannuation, 1800 RESPECT, Hearing Australia and more to be annuonced in the coming months (tailored for your specific region).
14-15 November : 6th Annual NHMRC Symposium on Research Translation.
The National Health and Medical Research Council (NHMRC) and the Lowitja Institute, Australia’s national institute for Aboriginal and Torres Strait Islander health research, are proud to be co-hosting the 6th Annual NHMRC Symposium on Research Translation.
This partnership indicates an alignment of priorities and a strong commitment from our two institutions to deliver a measurable, positive impact on the health and wellbeing of Australia’s First Peoples.
Under the theme “The Butterfly Effect: Translating Knowledge into Action for Positive Change”, the Symposium will be an opportunity to bring relevant expertise to the business of Aboriginal and Torres Strait Islander health research translation and put forward Indigenous perspectives that inform the most effective policies and programs. It will also be a forum to share knowledge of what successful research looks like at community level and what the key elements of success are.
We look forward to the participation of delegates with community, research and policy expertise, including outstanding keynote speakers Dr Carrie Bourassa (Canada) and Sir Mason Durie (New Zealand). We are confident that through our joint commitment to Aboriginal and Torres Strait Islander health research, the Symposium will make a significant contribution to the health of Aboriginal and Torres Strait Islander communities, families and individuals. This commitment also signals the importance of working together as equal partners, Indigenous and non-Indigenous.
15 -18 November :National Conference on Incontinence Scholarship Opportunity
The Continence Foundation of Australia is offering 10 scholarships to support health professionals to attend the 26th National Conference on Incontinence. The conference will be held in Sydney on 15-18 November 2017. The conference program and registration brochure can be found here.
This scholarship program is open to registered nurses and physiotherapists with an interest in continence care working in rural and remote areas of Australia. The scholarship includes full conference registration, including clinical workshops and social events, flights and accommodation. The top applicant also has the opportunity to participate in a placement at a Sydney continence clinic. Previous unsuccessful applicants are encouraged to apply.
14 December Shepparton One Day NATSIHWA Workshop VIC Forum
National Aboriginal and Torres Strait Islander Health Workers Association (NATSIHWA)
Join the National Aboriginal and Torres Strait Islander Health Workers Association (NATSIHWA) for a one day CPD networking workshop focussed on current workforce development opportunities.
Upskill and strengthen your skill level in a specialised area and find out what is happening through program development, education and funding opportunities.
Hear from organisations such as: PHN Primary Heath Network, CranaPlus, Autism QLD, Rheumatic Heart, PEPA Program of Experience in the Palliative Approach, Diabetes Australia, IBA Indigenous Business Australia, HESTA Superannuation, 1800 RESPECT, Hearing Australia and more to be annuonced in the coming months (tailored for your specific region).
11-12 April 2018 6th Rural and Remote Health Scientific Symposium Canberra call for extracts
About the Symposium
Drawing upon a tradition which commenced with the first rural and remote health scientific conference ‘Infront Outback’ held in Toowoomba in 1992, the 6th Rural and Remote Health Scientific Symposium will be held in Canberra, 11-12 April 2018.
The Symposium will celebrate 20 years since the establishment of the first university department of rural health in 1997 and will highlight the research and knowledge that followed this innovation.
Outback Infront will celebrate the leadership that has emerged from the rural and remote health research community, while at the same time, support early career academics and the next generation of rural health researchers.
The Symposium will focus on rural and remote health research that informs strategic health policy and health service challenges in rural and remote Australia.
The Symposium will provide an opportunity to share and develop research that seeks to understand and deliver innovative change through building evidence that has the potential to transform health outcomes and service delivery.
Who should attend
The Symposium program will be designed to engage academics, policy makers, expert researchers in rural and remote health and clinician-researchers, as well as emerging and early career researchers.
It will also be relevant to policy makers, university departments of rural health, rural clinical schools, research collaborations and bodies, rural workforce organisations and health services delivery networks and providers.
Program
As well as key presentations from respected researchers in rural and remote health the Symposium will also feature Rogano presentations (scholarly debate on a current research project that answer “how to” questions and encourage scholarly thinking and debate) and a return of the popular Lightning Talk presentations to support early career academics and the next generation of rural health researchers.
Abstracts are now being sought for general presentations, Lightning talks and Rogano presentations
” Sharing Cancer Australia’s Lots to live for video on social media will start a conversation between Aboriginal and Torres Strait Islander people about breast cancer and how early detection can save lives.
If you are an Aboriginal and Torres Strait Islander women, it is vitally important you know the normal look and feel of your breasts, the symptoms to look out for and the importance of seeing their doctor if you find a change.
Breast cancer is the most common cancer among women in Australia, including among Aboriginal and Torres Strait Islander women, yet Indigenous women are 16 per cent less likely to survive than non-Indigenous women.”
Professor Jacinta Elston ( breast cancer survivor ) Chair of the Cancer Australia Leadership Group on Aboriginal and Torres Strait Islander Cancer Control : She is a descendent of both the Kalkadoon people of North-West Queensland and the South Sea Islander people.
A new breast awareness video designed for Aboriginal and Torres Strait Islander women to share with family and friends on social media aims to increase early detection of breast cancer and improve survival.
Cancer Australia CEO, Dr Helen Zorbas, said the video, titled Lots to live for, had been produced to put vital knowledge about the importance of breast awareness and early detection of breast cancer in the hands of Aboriginal and Torres Strait Islander women and communities.
“Finding breast cancer early, while it is still confined to the breast, significantly increases the chances of survival,” Dr Zorbas said. “Early detection of breast cancer through breast awareness and increasing participation in mammographic screening are important ways to improve survival outcomes and address the disparity in breast cancer survival between Indigenous and non-Indigenous women.”
Professor Jacinta Elston, Chair of the Cancer Australia Leadership Group on Aboriginal and Torres Strait Islander Cancer Control, and an Aboriginal woman from Townsville, supported the video’s message and encouraged women to share it on social media.
“Studies have shown that social media has been used effectively in getting health messages out into our community,” Professor Elston said.
See opening message
“Aboriginal and Torres Strait Islander women aged between 50 and 74 years are also encouraged to have a free breast screen every two years. Mammographic screening is the best early detection test for reducing deaths from breast cancer.”
Professor Elston, who is herself a breast cancer survivor, acknowledged that some Indigenous women may be reluctant to discuss a breast change, due to shame, embarrassment, fear or stigma, but that this could seriously impact on their breast cancer outcomes.
“Changes in your breast may not be due to cancer, but if you find a change that is new or unusual, it’s important to see a doctor without delay,” Professor Elston said. “We need to look after our health – for ourselves and our families.”
The Lots to live for video, which features NITV’s Marngrook Footy Show presenter Leila Gurruwiwi, is designed to be easily accessible and shareable on social media platforms widely used by Aboriginal and Torres Strait Islander people.
“Cancer Australia is committed to improving cancer outcomes for Aboriginal and Torres Strait Islander peoples,” Dr Zorbas said.
Part 2 Key Facts Breast cancer in Aboriginal and Torres Strait Islander women
Key statistics
Incidence
• Breast cancer is the most common cancer among Aboriginal and Torres Strait Islander women.
• The number of breast cancer diagnoses among Aboriginal and Torres Strait Islander women increased by over 60% between the years 2004-08 and 2008-12.
Survival
• The breast cancer survival rate was 16% lower for Aboriginal and Torres Strait Islander women than for non-Indigenous women between 2006-2010.
Mortality
• Breast cancer was the second leading cause of cancer death among Aboriginal and Torres Strait Islander women after lung cancer (between 2007 and 2011).
• In 2010-2014, there were 154 deaths from breast cancer among Aboriginal and Torres Strait Islander women in Australia.
Factors affecting breast cancer outcomes among Aboriginal and Torres Strait Islander women
Aboriginal and Torres Strait Islander women:
• are less likely than non-Indigenous women to have a screening mammogram
• may choose not to visit a doctor when they notice changes in their breasts.
• are less likely to undergo cancer treatment
• are less likely to complete cancer treatment
• are more likely to have 1 or more other health problems such as heart disease and/or diabetes.
As a result of these factors, breast cancer may be more advanced when diagnosed.
Key messages
Finding breast cancer early
1. Breast awareness and early detection of breast cancer for Aboriginal and Torres Strait Islander women
• Finding breast cancer early means there are more treatment options and the chances of survival are greatest.
• More than half of breast cancers are diagnosed after a woman or her doctor notices a change in the breast.
• This shows how important it is that women are aware of the normal look and feel of their breasts and are confident in reporting unusual breast changes.
How can Aboriginal and Torres Strait Islander women get to know the normal look and feel of their breasts?
• Women of all ages, daughters, mothers, aunties and grandmothers, are encouraged to get to know the normal look and feel of their breast.
• They don’t need to be an expert or know a special way to check their breasts. They can do this as part of everyday activities such as dressing, looking in the mirror, or showering.
Changes to look out for
There are a number of changes to look out for:
• A new lump or lumpiness
• A change in the size or shape of your breast
• A change in the nipple
• Discharge from the nipple
• Any unusual pain
• A change in the skin of your breast
What to do if women find a change?
While most breast changes are not due to cancer, if a woman finds a change in her breast that is new or unusual for her, it’s important to see a doctor without delay.
Screening mammograms
• Aboriginal and Torres Strait Islander women aged between 50 and 74 years are encouraged to attend mammographic breast screening every two years. Mammographic screening is the best early detection test for reducing deaths from breast cancer.
Where to go to have a breast screen?
BreastScreen Australia provides free breast screening for women 50-74 years and has services in all states and territories. To find out more call 13 20 50.
Lots to Live For!
Cancer Australia’s new video Lots to Live For was developed to put vital knowledge about the importance of breast awareness and early detection of breast cancer in the hands of Aboriginal and Torres Strait Islander women and communities.
The Lots to Live For video, which features Marngrook Footy Show presenter Leila Gurruwiwi, is designed to be accessible and shareable on social media platforms widely used by Indigenous communities.
” When delegates from the Dialogues assembled at Uluru in May this year, the exhaustive deliberations and informed participation through the Regional Dialogues led to a broad consensus, as articulated in the Uluru Statement from the Heart which was adopted by the Convention.
Specifically, Australia’s First Peoples overwhelmingly rejected any purely symbolic changes to the Constitution, such as through a ‘statement of recognition’.
……..Dialogue participants and the Uluru Convention showed significant agreement.
There was overwhelming consensus around three proposals.
First, for a constitutionally established representative body that would give First Nations a Voice directly to the Federal Parliament.
Second, for the establishment of a Makarrata Commission to supervise the making of Treaties with us.
Third, for a process of local and regional Truth-telling which could form the basis for genuine reconciliation.”
Ms Pat Anderson AO delivered the 17th Annual Vincent Lingiari Memorial Lecture at Charles Darwin University on Wednesday, 16 August.Full Text and video below
The lecture commemorated the historic walk-off from Wave Hill Station by Indigenous stockmen and their families, planting the seeds for Aboriginal land rights in Australia.
For her lecture titled: “Our Hope for the Future: Voice. Treaty. Truth” Ms Anderson reflected on her personal history and experience as an advocate for social justice during the last half-century of struggle for the recognition of the rights of Aboriginal and Torres Strait Islander people.
Chair of the Lowitja Institute and co-chair of the former Prime Minister’s Referendum Council, former Chair of NACCHO and CEO of Danila Dilba ACCHO and AMSANT , Ms Anderson is a campaigner for advancing the rights of Aboriginal and Torres Strait Islander people in education, health, early childhood development, and violence against women and children. She is an Aboriginal advocate for social justice and winner of the 2016 Human Rights Medal.
Ms Pat Anderson AO delivered the 17th Annual Vincent Lingiari Memorial Lecture at Charles Darwin University on Wednesday, 16 August, which commemorated the historic walk-off from Wave Hill Station by Indigenous stockmen and their families, planting the seeds for Aboriginal land rights in Australia.
Good evening everyone,
I acknowledge and pay respects to the Larrakia people, traditional custodians of the land on which we are meeting tonight.
I want to thank Charles Darwin University for asking me to deliver this Lecture. This is huge honour for me. It’s always hard presenting in your home town.
I was feeling a bit anxious about that because you all know everything about me.
I would like to acknowledge Wendy Ludwick who I think put my name forward for this honour.
We are here to honour the memory of Vincent Lingiari and his leadership in the 1966 Wave Hill strike.
I will return to that story, and to the place of the Gurindji in the contemporary struggle for the rights of Australia’s First Peoples shortly.
But first, I’d like to share another story with you, a personal story.
This story is from the 1950s, a decade before the Wave Hill Walk Off, and is set at Parap Camp a few miles from here (in the suburb now called Stuart Park), where I and my sisters grew up with our mum and dad.
For those who don’t know the history, Parap Camp was home to many Aboriginal and some Torres Strait Islander families in those harsh post-War years.
Many of those families had a Stolen Generations heritage, with the parents of Parap camp families having grown up in the nearby Kahlin Compound. Kids were rounded up from all over the Territory.
My mother was one of those, taken as a young girl sometime in the 1930s by white men on horseback from her Alyawarre family north east of Alice Springs.
She was brought here to the Compound, fifteen hundred kilometres away.
After growing up at Kahlin, she was sent to work as a young teenager on a farm on the other side of the Darwin harbour, near Belyuen.
Later, she met my dad, a Swedish merchant seaman who had jumped ship in Fremantle, and made his way to Darwin.
They married and settled at Parap Camp.
My story is from when I was about 9 or 10 years old, when I was in Grade 3 or 4 – like almost all children from Parap Camp, I and my sisters attended school without fail.
School attendance was non-negotiable in those days – we all just went.
Every year the class would have a Christmas Party at the end of the final term, and the idea was that all the kids would bring food from home for the party.
I was excited because I knew my mum made the best sponge cakes ever: great high, fluffy things.
I pictured myself taking one of these cakes into school – I was a bit vain, and wanted to show off what a great cook mum was.
But when I asked her to make the cake, she flatly refused.
No matter what I said, how I nagged at her, she just said no.
Finally, in frustration, I just burst out: “But why mum? Why won’t you make one of your cakes and let me take it to the school party?”.
She hesitated for a moment.
And then she said quietly: “I don’t like white people eating my food”.
I knew immediately from the way she said it that not only was this the end of the argument, but also that she was telling me something more.
I can still see her face and hear her voice.
I haven’t forgotten this: although I didn’t understand how at the time, it was clearly important.
And so I had to trudge off to my Christmas party with a packet of store bought biscuits, while all the other kids brought scones, cakes and biscuits baked by their mothers – none of which, I might add, were as good as what my mum could have made.
This sounds like an ordinary domestic, family event.
And it is.
But like so many stories that are part of every Aboriginal family in this country, there is a lot packed into this little scenario.
For a start, how did my mum get to be so good a cook?
I see now that her skill with cooking was something she had learnt from the white women she worked for as domestic, unpaid labour.
Her ability to cook a beautiful sponge cake was a direct consequence of the policy of assimilation by which all Australian governments aimed to eradicate us as distinct cultural groups.
At the same time, there were other skills that were withheld from her and so many other Stolen Generations.
Most importantly, growing up in Kahlin Compound she was never taught to read or write.
Despite the rhetoric about Aboriginal children being taken away to improve their chances in life, literacy was one skill that the administration clearly thought was of no use to a young Aboriginal woman.
That much is clear from our history.
However, on a personal level, much about my mother’s motivations in the story about the cake remains curious to me.
Did she not want white people to eat her food as an act of defiance?
Was it a reluctance – or a refusal – to place herself in a situation of being judged by them?
Was it her own brand of passive resistance?
I don’t know.
However, I do know it was a profound moment in our relationship as she revealed something of herself to me.
This moment has stayed with me over all these years.
And I believe this little incident points to the great gulf in experience between Aboriginal and non-Aboriginal Australia.
It points towards an experience carried by so many of our families: the experience of having been treated unjustly, but of that injustice not being acknowledged.
This experience has been analysed by Jill Stauffer in her 2015 book, Ethical loneliness: the injustice of not being heard1.
Stauffer describes the profound isolation and loneliness that arises as a consequence of such an experience.
Calling it ‘ethical loneliness’ she says that it is a condition undergone by persons who have been unjustly treated … who emerge from that injustice only to find that the surrounding world will not listen to or cannot properly hear their testimony. … ethical loneliness is the experience of having been abandoned by humanity, compounded by the experience of not being heard.
There is something of this ethical loneliness in my mother’s experience, and even in the story of the cake she would not make.
I believe that experience is common to many if not all Aboriginal and Torres Strait Islander families.
It stems from the complex, often damaged and damaging relationship between our First Nations and those who colonised this place from 1788 onwards.
Much of that damage remains embedded in the relationship between black and white Australia.
This nation has never properly dealt with that damage.
It has never properly acknowledged it, and acted upon that acknowledgement.
I believe we now, in 2017, all of us over the age of 18, this generation, have an historic opportunity to do that, to begin the process of repair, to re-set that relationship on a foundation of equality, justice and truth.
That opportunity is presented by the prospect of genuine and substantive reform to the Australian Constitution, and that is the topic I want to talk to you about this evening.
I would like to take you on the journey that I have been recently on as a member of the Referendum Council, which was tasked with making recommendations to the Federal Government on constitutional reform.
I would like to share with you our experience of the unique regional Dialogues with First Peoples and communities, and what we heard in them, culminating in the National Convention of First peoples at Uluru in May this year, and the Uluru Statement from the Heart.
And most importantly I want to describe the three essential demands to come from this process, which I summarise with these three words:
Voice.
Treaty.
Truth.
Before we trace that journey from the world of the Parap Camp in the 1950s, to where we stand today in 2017, I would like to acknowledge the importance of the Wave Hill Walk Off in 1966 in our history.
Mr Lingiari and the other Gurindji men and women first walked off their jobs on the Wave Hill station to demand fair pay and conditions, but ended up sitting down at Wattie Creek and demanding the return of their traditional lands.
They were demanding proper acknowledgment of the injustice done to them, and proper restitution of the harms done.
In doing so, they began the modern land rights movement.
But they were also re-asserting the struggle for self-determination, as summed up so elegantly by Mr Lingiari himself when he said:
“We want to live on our land, our way”
In those nine words, he captured the essence of what have been and continue to be the central demands of our First Nations since 1788.
First, recognition of our sovereignty, never ceded, of the land, of Country.
Second, acceptance of our right to continue in our unique and diverse cultures.
The Gurindji and Mr Lingiari powerfully re-asserted those demands, just as our First Nations have done since the beginning of the colonisation of Australia, and just as we have continued to do since.
This year, 2017, is a year of anniversaries of events which built upon and extended the rights of First Peoples as so clearly stated by the Gurindji.
It is
• 50 years since the 1967 Referendum;
• 25 years since the Mabo decision overturned the lie of ‘terra nullius’ in 1992; and
• 20 years since the Bringing Them Home Report in 1997.
It is also, crucially, 10 years since the Intervention was unleashed on our communities here in the Northern Territory.
The Intervention was the counter-revolution, the attempt to turn back the clock to the times before the Gurindji and Wave Hill, and the 1967 Referendum, and all the other achievements.
The Intervention was the attempt to take us back to the world of Parap Camp in the 1950s, when the powers of the nation-state reached into every aspect of how we lived our lives.
Now, ten years on, it is clear how profoundly and utterly the Intervention and the thinking behind it has failed.
It continues, however, to create much heartache and pain.
As John Lawrence in his recent Castan Centre Address3 has stated, tem years on, the Northern Territory gaols more people per capita than any country in the world.
The overwhelming majority of those incarcerated are Aboriginal.
The number of children being removed from their families is soaring: it rose by an average of 16% per year between 2011 and 2015.
This frightening increase is entirely due to the removal of Aboriginal children from their families4.
Family violence is out of control.
These figures – which many of you will know – are profoundly disturbing.
They demonstrate the tsunami of anger, frustration, despair and sadness that is engulfing our communities and families.
These type of figures are echoed across the country.
They reflect the kind of Intervention-thinking that has informed policy making over the last ten years, based on the idea that the nation-state knows best what is good for us.
Let us remember that the Intervention was trumpeted by its instigators as necessary to protect Aboriginal women and children.
It marked a shift in policy-making not just here but across the country.
Intervention-thinking sees self-determination as a failed idea, and blames us for the situation in which we find ourselves.
It believes that we do not have anything to offer, that we are at best ‘risks’ to be managed.
It ignores or condones or covers up the abuse of young people in detention, or our lack of housing or access to education.
I say again: it has utterly failed.
We can see this through the statistics, but more importantly through visiting many of our communities and listening to the experience of Aboriginal and Torres Strait Islander peoples over these last few months.
I’ve been working in this field all of my adult life, and I can say honestly say that I have never seen things so bad.
This has to change.
We now sit in 2017 at what I believe is a critical junction in our history, not just for the First Nations of this country, but for the nation-state as a whole.
Six weeks ago, the Referendum Council of which I was Co-Chair handed a report to the Prime Minister, recommending what constitutional change should look like if it is to be acceptable to our First Peoples.
The report documents what we were told in a series of regional dialogues with Aboriginal and Torres Strait Islander people and communities across the country.
Going out and talking to Aboriginal and Torres Strait Islander people was our first priority under our terms of reference.
These twelve regional Dialogues were held from Thursday Island to Hobart, from Perth, to Ross River outside Alice Springs, to Sydney and Melbourne. People from across the regions came to these centres.
We also held a one-day information session in Canberra.
Each Dialogue was attended by around one hundred people, including Traditional Owners, representatives of local organisations, and individuals.
Each was held over three days to allow full consideration of a number of proposals for Constitutional reform. It was the same format and same agenda for each Dialogue. We needed a methodology which could, in some way, be empirically measured.
The reforms that each Dialogue considered had been inherited by the Referendum Council from the work of the Expert Panel on the Recognition of Aboriginal and Torres Strait Islander Peoples in the Constitution (co-chaired by Patrick Dodson and Mark Leibler) and the Joint Select Committee on Constitutional Recognition of Aboriginal and Torres Strait Islander Peoples (co-chaired by Senators Ken Wyatt and Nova Peris).
They were:
• first, a statement acknowledging us as the First Australians, either inside or outside the Constitution;
• second, amending or deleting that part of the Constitution which empowers the Commonwealth to make laws for Aboriginal and Torres Strait Islander peoples;
• third, inserting a guarantee against racial discrimination into the Constitution; and
• fourth, deleting that part of the Constitution which contemplates the possibility of a state government excluding some Australians from voting on the basis of their race.
The Dialogues also considered a fifth option, that of a First Peoples’ Voice to be heard by Parliament, and the right to be consulted on legislation and policies that affects us.
The Dialogue process was unprecedented in Australia’s history: never before have we as First Nations sat down across the nation in such an intensive, structured manner to deliberate on constitutional matters.
It was a passionate process.
Delegates grappled with the technical and legal implications of these proposals, as well as with their political viability.
There were disagreements, there were even arguments: how could it be otherwise when 1,200 people from all the diversity of our Nations were brought together to talk about matters so closely connected with the experiences and history of their families, clans and communities?
But there was also an extraordinary level of agreement on some matters.
When delegates from the Dialogues assembled at Uluru in May this year, the exhaustive deliberations and informed participation through the Regional Dialogues led to a broad consensus, as articulated in the Uluru Statement from the Heart which was adopted by the Convention.
Specifically, Australia’s First Peoples overwhelmingly rejected any purely symbolic changes to the Constitution, such as through a ‘statement of recognition’.
There were two reasons behind the rejection of this narrow model of Constitutional recognition.
First, there was a concern that formal recognition in the Constitution might interfere with sovereignty – and all Dialogues were steadfast in asserting the fact that we as First Nations had never ceded our sovereignty.
In re-asserting the fact of sovereignty, the delegates echoed the conclusions of the Expert Panel on Constitutional Recognition of Aboriginal and Torres Strait Islander Peoples five years ago, which stated that5:
The … occupation of the country … proceeded on the fiction of terra nullius. It follows that ultimately the basis of settlement in Australia is and always has been the exertion of force by and on behalf of the British Crown. No-one asked permission to settle. No-one consented, no-one ceded. Sovereignty was not passed from the Aboriginal peoples by any actions of legal significance voluntarily taken by or on behalf of them.
Second, and more simply, participants in the Dialogues and at Uluru simply did not trust the likely process for drafting a constitutional statement of recognition
The concern was that by the time the lawyers were through with it, such a statement would end up being so bland as to be incompatible with the duty to recognise the difficult truths of Australia’s past.
Instead, our mob wanted substantive change, structural reform, for their communities on the ground.
And if it didn’t fit that criteria, they weren’t interested.
And this is where Dialogue participants and the Uluru Convention showed significant agreement.
There was overwhelming consensus around three proposals.
First, for a constitutionally established representative body that would give First Nations a Voice directly to the Federal Parliament.
Second, for the establishment of a Makarrata Commission to supervise the making of Treaties with us.
Third, for a process of local and regional Truth-telling which could form the basis for genuine reconciliation.
These three things – Voice – Treaty – Truth – were the key consensus demands that arose from the Dialogues, were captured in the Uluru Statement from the Heart, and form the core of the Referendum Council’s report.
I’d now like to turn to each of these three crucial concepts and unpack them, give you my view why they are important, what they might mean, and how they might provide a pathway out of our current situation.
These are not abstract notions, or intellectual constructs.
Changing the Constitution, many of us believe, is the only place left for us to go.
We have sat on the Committees, we have set up our own organisations, we have changed national policy agendas, but we still haven’t been able to achieve the substantive change demanded by our communities.
As Marcia Langton said at Garma recently, we have been Royal Commission-ed out, we have been committee-ed out, and we have been panel-ed out.
We still have to rely on other people’s good will.
And that is not good enough anymore.
We need more than that.
We need once and for all for our sovereignty to be recognised and our voices to be heard.
The recommendation for substantive constitutional change was for the establishment of a “representative body that gives Aboriginal and Torres Strait Islander First Nations a Voice to the Commonwealth Parliament”.
We believed – following the consensus at Uluru – that this is the only constitutional reform which would accord with the wishes of Aboriginal and Torres Strait Islander peoples.
Why is this important?
Establishing such a body in the Constitution has both substantive and symbolic value.
Symbolically, it recognises the unique place of First Peoples in Australian history and in contemporary Australian society.
It formally acknowledges our place here.
In asking Australians to vote ‘yes’ to such a proposal we would be asking us all to reflect on who we are, on what values and principles we hold dearest.
It would establish a significant national narrative about working together – about a genuine two-way conversation.
But such a body will also provide substantive benefits.
A constitutionally entrenched Voice to Parliament could address Australia’s poor history of consultation with our Peoples by government.
All too often we have been excluded from the key decisions that are made about our lives.
The Intervention itself is a key example, designed over three days6, in some offices in Canberra by people who took little account of the evidence, had no understanding of the realities of our lives and most significantly didn’t talk to any of us.
(No wonder it has failed!)
The Voice to Parliament would ensure we have input at the highest level into the policy-making that affects us.
It could also play a valuable monitoring role.
Properly resourced, it could hold Government to account, regularly reviewing and reporting on the implementation of recommendations from the host of inquiries and reports from the Royal Commission Into Aboriginal Deaths In Custody onwards.
It could also monitor the use of the Constitution’s ‘race power’ or attempts to suspend racial discrimination legislation so that measures like the Intervention could be properly scrutinised before their implementation.
Embedding the establishment of the Voice to Parliament in the Constitution is vital because the body’s existence would not then be at the whim of whichever government was in power in Canberra.
You know, every time there is a change of government, or a new Minister, or even a Head of Department, we all have to troop down to Canberra yet again and justify our existence. Pretty much, start all over again.
The Voice to Parliament would be a permanent and enduring feature of the nation’s body-politic.
It could only be abolished by going back to you, the people, in a new referendum.
To date, all our national organisations have disappeared with the stroke of a Minister’s pen.
We would be, at last, in the main building, not in the demountable out the back.
Of course, the details of how to establish such a body would need to be carefully negotiated with Parliament once its establishment was agreed through Referendum.
My vision – and that of many people we spoke to during the dialogues and at Uluru – is for a body that include representation from all the diversity of First Nations across Australia.
It would be a place for dialogue, a meeting place for us and with us.
And in my opinion, it is this diversity that would enrich the body-politic.
After 65,000 years or more on this continent, with all our different languages, histories and cultures, I think we would have something powerful and unique to offer the nation-state through such a body.
Let me turn to second proposal to come from the Dialogues and from Uluru: Treaty.
Australia is one of the few liberal democracies around the world which still does not have a treaty or treaties or some other kind of formal acknowledgement or arrangement with its Indigenous minorities.
It is something we have demanded since at least the mid-nineteenth century.
Despite the hard-won gains, such as through the Land Rights Act following the Gurindji Walk Off, and the Native Title Act sparked by Eddie Mabo, there is unfinished business that we need to resolve.
We used the word ‘Makaratta’ to describe this process of agreement or Treaty-making.
Makaratta is the process that guides the Yolngu Nation in North East Arnhem Land through difficult disputes, and its workings have been recently described by Galarrwuy Yunupingu in this way7:
… each party, led by their elders, must speak carefully and calmly about the dispute. They must put the facts on the table and air their grievances … The leaders must always seek a full understanding of the dispute: what lies behind it; who is responsible; what each party wants, and all things that are normal to peacemaking efforts. When that understanding is arrived at, then a settlement can be agreed upon.
Following the Uluru Statement, this means the establishment of a ‘Makarrata Commission’ to set up a national Framework and principles for negotiating treaties, and a possible a national settlement document.
A Treaty is a pathway to the recognition of sovereignty and to the achievement of self-determination.
It is an agreement between equals.
Such treaties could be regional or State-wide, and it would be the Makarrata Commission’s job to provide a national framework for, and supervise, these two-way processes.
Critically, treaties are inseparable from the third demand from the Dialogues and Uluru: Truth.
You cannot make a lasting and effective agreement unless you have a shared, truthful understanding of the nature of the dispute, of the history, of how we got to where we stand.
The true story of colonisation must be told, must be heard, must be acknowledged.
Because, this is still not the case.
This is difficult and painful territory – for us as well as for mainstream Australia.
It can be hard to hear.
As Jill Stauffer says in her book ‘Ethical Loneliness’ that I quoted from at the beginning of tonight:
Responding well to others, especially survivors of wrongdoing, may require that we open ourselves to hearing something other than what we expect or want to hear
But hearing this history is necessary before we can come to some true reconciliation, some genuine healing for both sides..
I was reminded of this just last month when I read media stories about an online digital map of more than 150 massacres developed by Professor Lyndall Ryan at the University of Newcastle8.
Through meticulous examination of the records, the map seeks to provide the evidence for those who still question whether massacres happened.
Professor Ryan has started documenting these facts for the eastern coast of Australia but plans to extend this to the rest of the country.
This is important work.
But I question how it is that we have had to wait until 2017 for this?
Why is this not part of the national conversation?
Our communities know about the massacres.
Our families know about the children being forcibly removed from their families.
But it seems that there is a need for many in mainstream Australia to pretend that all this didn’t happen, that it’s all just part of a ‘black armband’ view of history, made up to make you feel guilty.
One of the most moving episodes in the regional dialogues for me personally came at Ross River near Alice Springs.
There the Elders spoke of the distress they felt at the recent placement of a statue of the explorer John McDouall Stuart in Alice Springs to mark the the 150th anniversary of his attempt to reach the Top End from Adelaide.
The statue was shown holding a gun.
The Elders felt legitimately that this showed a painful lack of respect, given the fact that Stuart’s journey led directly to a series of massacres in the region as control of the land was wrested from the traditional owners.
Let me be clear: this process of truth–telling is not about guilt.
Guilt is a debilitating emotion that stops us moving forward or doing anything.
What I’m talking about is respect and acknowledgment.
As one participant in the Regional Dialogues in Broome said:
[We are] people who worked as stockmen for no pay, who have survived a history full of massacres and pain. We deserve respect.
And of course, this is not just the history of our First Peoples – it is the history of all of us, of all of Australia, and we need to own it.
Then we can move forward together.
The Dialogues opted for the development of a ‘Declaration of Recognition’ to be passed by all Australian Parliaments.
This declaration – outside the Constitution – would be free to articulate that difficult shared history.
It could provide a unifying statement about the three waves of people who make up the Australian story:
• our ancient First Peoples (65,000 years or more),
• those people who came in 1788 and after,
• the peoples who have come from out of Europe and Asia and who continue to try to come us today, often fleeing persecution and seeking a better life.
Three waves of people.
So, this where we stand now in 2017.
The unprecedented process of deliberation by Australia’s First peoples, through the regional Dialogues and at Uluru, led to the formulation of three clear demands:
Voice.
Treaty.
Truth.
Some commentators and others have expressed concern that these are new proposals, the examination of which will need yet more new processes to consider.
I respectfully disagree.
None of these issues are new.
We have been talking about these things for a long time.
Other commentators believe that these are impractical, left-field proposals.
Again, I respectfully disagree.
I believe these changes are challenging but achievable, and are proportionate to the level of distress, anger and powerlessness being felt in our communities.
In the international landscape of recognising Indigenous peoples, what we are asking for is modest, conservative even.
Many of our First Nation communities and families are plagued by a myriad of challenges including poverty, suicide, youth detention, family breakdown, and all kinds of health problems.
Worse, in my view, than any of this, is that too many of us feel hopeless.
To reverse this and to take our rightful place in this country, we need to create new places, new ways by which we can speak and get things done to deal with our complicated 21st century lives.
At the same time we will strongly and even fiercely guard who we are and our right to be different.
We need to create a future when we, and our children and grandchildren, are recognised as having something powerful and unique to offer this nation.
This needs to happen now, and not just for us as First Nations.
This is about the social and emotional wellbeing of the country as a whole.
It is a time of reflection, a time for all Australians to consider what kind of a society we are today, what are our values and our principles.
Surely, we are not the same people as we were in 1901 when the Constitution was drawn up.
Eventually we will have to sit down together, black and white in this nation, and deal with this.
For the truth is that this is our place.
We, the First Nations, are not going anywhere.
They can put it off for another ten years, twenty years fifty years.
But eventually you will have to sit down with as respectful equals and sort out this relationship.
But right now, we have an opportunity, a roadmap for doing that.