” Let us not forget that major policies that wreak havoc on communities — like the Northern Territory Intervention and the cashless welfare policies — were enacted with bipartisan support.
While Dodson is a strong voice against laws and policies that harm our people, we cannot ignore that he belongs to a party that has a long history of harming us and voting in favour of policies introduced by the other major party, which harmed us also, under the guise of “for our own good”.
It is disingenuous to lay the fault for oppressive policies solely at the feet of the Coalition, because Labor had their hand in supporting these policies and, in some instances, expanding their scope. Labor has a lot to answer for and only meaningful change can ever address the historical atrocities committed by this organisation.
Labor has not only been historically responsible for policies that oppressed our people but they have been complicit in contemporary oppressive policies “
On Pat Dodson, Labor’s paternalism and avoiding lip service NATALIE CROMB
Gamilaraay woman and Indigenous affairs editor, Independent Australia. Crikey
In the final week of the Election 2019 campaign this is the first of our series “Who will be the Minister for Indigenous Affairs and Minister for Indigenous Health for incoming Government after 18 May ” We welcome your feedback in comments below
“ Our Shadow Cabinet, guided by our First Nations’ Caucus Committee, has identified targeted and focused initiatives, launched today, that will bring the vision of justice and fairness to the lives of First nations’ peoples.
In education, we have many new and powerful initiatives that work directly to build bridges for the futures of our young people.
Our unprecedented investments in Indigenous health will be community designed and delivered, more than ever before.
Our new policies and programs in the environment will help visitors to understand the complex national cultural web from which our landscapes arise from.
It will be a challenge for us, to do all we have set out in our new policies and programs.
But we will work to achieve that.
We want to be the party of choice for First Nations Peoples “
Senator Patrick Dodson speaking at the Australian Labor Party national launch in Brisbane Sunday full speechHERE and Download policy Document
I have been asked by many about my thoughts on Pat Dodson potentially being minister for Indigenous affairs.
As an outspoken black woman, you best believe I have thoughts — many.
Do I think this is a good thing? Yes. Do I think this is the answer? Hard no on that one.
I am not here to rubbish Dodson, he has a lengthy track record of seeking change for our people. But he is part of the political machine.
He is part of a major party and is beholden to policies drafted about us without us, and because of that I view this announcement by Bill Shorten with the cynicism that is necessary for black fullas.
It is difficult not to be caught up in the exciting prospect of having an Indigenous person holding the role of Indigenous affairs minister after so many years dealing with the farce that has been Nigel Scullion and Tony Abbott but it is essential that we stow our celebrations and consider what this really means in politician speak.
Shorten’s promises
The clue in why we need to be reserved lies in the language of the announcement that Bill Shorten made. Shorten said that paternalism and top-down approaches had failed, which is correct. He also said that “we want to try something different if we get elected”, and stated further “we want to try the idea of Aboriginal-controlled organisations making decisions”.
We need to remember that the words used by politicians are very deliberate, considered and rehearsed. So when Shorten says we “want to try” it sends off alarm bells in my head — he is using this appointment and manner of policy roll-out as an experiment and we are the subjects of this experiment. You might think I am jumping at shadows and consider this rather innocuous but this language and approach is a maintenance of the deficit dynamic.
Bill Shorten does believe he is making a genuine and positive announcement but he doing this from a position of privilege and one where he has not considered change beyond policy roll-out. He has not considered that the issues affecting communities are not “problems” — they are consequences. He has not considered systemic reform to address the failure that is colonisation and the institutions resultant.
What Labor needs to do next
Consequently, it is essential that our support of this announcement be contingent upon it not being mere lip service and change goes beyond merely the manner of policy delivery.
If elected, Labor as a party and as a government needs to have their policies crafted by First Nations drafts people following community consultations with the very communities affected.
Policies should not be broad-brush either; they need to start seeing us for the diverse and vast communities we are. It is not unreasonable for a policy — at the request of the community — to apply solely to that community. Applying a “one size fits all” approach needs to go out the window, along with the viewpoint that we are a problem that needs to be solved.
This announcement does not change anything and we need to remember this and resist tokenism.
Shorten’s announcement is a good one and I do not want to diminish the pride we will all feel when we have one of our own heading up this portfolio. However, the appointment is merely tokenistic if it does not empower Dodson to make structural changes to the way this portfolio operates and to a Labor government should it be elected.
Unless Labor changes the way it operates as a party then this new approach will fail and that failure will be put at the feet of Dodson.
Make no mistake, unless there is change from within the institutions that “govern” this country, all that is happening here is paternalism repackaged. If the intent is to maintain the policies that oppress our people and communities but change the way in which the policies are rolled out, this is simply getting black bodies to do the work of white decision makers. Shorten is not suggesting systemic change here, he is suggesting a change in approach with the delivery of policies — not the policies themselves and herein lies the issue.
While I back Shorten’s announcement, I call upon him and his party for more. Think bigger, more than 200 communities bigger, and then you may grasp how utterly out of your depth you are and see the value in self-determination.
We are not homogenous and have resisted colonial assimilation for over 200 years, perhaps we might know a little something about survival under the worst conditions, and perhaps we could teach a thing or two about how to make this country thrive.
Let me tell you: what we have to teach has nothing to do with capitalism.
NACCHO has developed a set of policy 10 #Election2019 recommendations that if adopted, fully funded and implemented by the incoming Federal Government, will provide a pathway forward for improvements in our health outcomes.
The current health outcomes for Aboriginal and Torres Strait Islander people are unacceptable. 65% of Indigenous people live in rural Australia.
We are calling on all political parties to include these 10 recommendations in their election platforms and make a real commitment to improving the health of Aboriginal and Torres Strait Islander peoples and help us Close the Gap.
Our ACCHO TOP 10 key asks of a new Federal Government
“ It’s fantastic to welcome 72 new LDATs to the program who will develop and deliver local plans and activities to prevent alcohol and drug misuse in their local communities.
Today’s announcement brings the total number of LDATs to 244 across Australia, exceeding our target of 220 by 2020.
LDATs bring together community organisations to tackle substance misuse which can have devastating impacts on our communities – especially in rural and regional areas – and it’s clear that our communities are increasingly becoming empowered to take action at the local level.
The LDAT partnerships include local councils, service providers, schools, police, young people, Indigenous and primary health services and other non-government organisations, and the teams will have support from the Alcohol and Drug Foundation to assist in prevention activities,”
Minister for Regional Services, Senator Bridget McKenzie
May 2018 : The Senator with Alcohol and Drug Foundation CEO Dr Erin Lalor and General Manager of Congress’ Alice Springs Health Services, Tracey Brand in Alice Springs talking about the inspirational Central Australian Local Drug Action Team at Congress and announcing 92 Local Drug Action Teams across Australia building partnerships to prevent and minimise harm of ice alcohol & illicit drugs use by our youth with local action plans
Part 1 Press Release
Speaking at the Wellington LDAT site in Sale, Victoria, the Minister for Regional Services, Senator Bridget McKenzie today congratulated the local community organisations, along with their partners, that will receive funding from the Federal Government through the fourth round of the successful Local Drug Action Team Program.
The new LDATs are being supported through the $298 million investment under the National Ice Action Strategy to combat drug and alcohol misuse across Australia.
Each of the 72 LDATs will receive an initial $10,000 to help them to refine a local community action plan. Each team will have an opportunity to apply for additional funding to support the delivery of local activities once their plans are finalised.
The Member for Gippsland Darren Chester welcomed today’s funding announcement.
“It’s important that we try to stop people in our community from trying illicit drugs for the first time and reduce binge drinking and alcohol abuse,” Mr Chester said. “One way of doing that is to ensure that everyone feels they are part of the community.”
”Gippsland is no different to other areas and drugs and alcohol are ruining lives and devastating families. Ice and other drugs do not discriminate.
“Many of us personally know families in our community who are dealing with the fallout of these insidious drugs.
“This funding enables the community to band together to fight the problem.”
Minister McKenzie said the LDATs announced will be supported to identify and deliver evidence based prevention, promotion and harm-reduction activities which will work for their local community.
Minister McKenzie acknowledged the importance of LDATs for driving change at a local level and highlighted the great work coming out of the program.
“The Hepburn LDAT, for instance, in Victoria is working to prevent and minimise harm from alcohol and drug misuse by improving access to education and skills development for young people,” Minister McKenzie said.
“The team has developed a 19-week program to up-skill young people and help them to build confidence, improve their knowledge about health and reconnect with their community.”
The Local Drug Action Team Program is a key component of the National Ice Action Strategy.
For free and confidential advice about alcohol and other drugs treatment services, please call the National Alcohol and Other Drug Hotline on 1800 250 015.
Alcohol and other drug-related harms are mediated by a number of factors – those that protect against risk, and those that increase risk. For example, factors that protect against alcohol and other drug-related harms include social connection, education, safe and secure housing, and a sense of belonging to a community.
Factors that increase risk of alcohol and other drug-related harms include high availability of drugs, low levels of social cohesion, unstable housing, and socioeconomic disadvantage. Most of these factors are found at the community level and must be targeted at this level for change.
Alcohol and other drugs are a community issue, not just an individual issue. Community action to prevent alcohol and other drug-related harms is effective because:
the solutions and barriers (protective/risk factors) for addressing alcohol and other drug-related harm are community-based
it creates change that is responsive to local needs
it increases community ownership and leads to more sustainable change
We encourage Local Drug Action Teams (LDATs) to link with and/or build on existing activity approaches that have been shown to work.
Select an existing evidence-based activity
Existing activities may have an alcohol and other drug focus, or possibly a different overall focus such as preventing gambling harm, or enhancing mental wellbeing. Be prepared to look outside the alcohol and other drug sector for possible approaches; for example, activities that share a focus on strengthening communities to improve other health and social outcomes.
A limited number of existing activities are listed below. You may also find other activities through local health services, peak bodies and by drawing on local knowledge and networks you have access to.
Existing strong and connected community activities in Australia:
Delivered by the Alcohol and Drug Foundation , the Good Sports Program works with local sporting clubs across Australia to provide a safe and inclusive environment, where everyone can get involved. The activity has run for nearly two decades and is proven to reduce harm and positively influence health behaviours, as well as strengthen club membership and boost participation.
Community Hubs provides a welcoming place for migrant women and their children to learn about the Australian education system. With strong evaluation to support the effectiveness of the program, Community Hubs focuses on engagement, English, early-years and vocational pathways.
A national organisation that uses sport and art to improve the lives of people experiencing complex disadvantage.
If you have found some existing activities that could be incorporated, it is useful to seek out further information to find out if it is relevant.
You might want to consider the following questions (some answers may be available online, others you may have to seek directly from the organisation):
Does the activity align with your community needs?
Is the activity available in your geographic area? If face-to-face delivery is not available, is remote access an option?
Has the activity been shown to be effective at strengthening community cohesion and connection, and reducing and preventing alcohol and other drug-related harms? What evidence is available to demonstrate this?
Due to the limited number of existing activities available and the need for tailored approaches, many Local Drug Action Teams will work with partners to develop and deliver a targeted activity in their community. Review the paragraph below d. Determine resources required and Map your steps for insight into what is required when developing new approaches.
International Women’s Day (IWD) will be celebrated today across all our 304 Aboriginal community controlled health clinics and 8 affiliates , where thousands of Aboriginal and Torres Strait Islander woman are involved daily in all aspects and levels of comprehensive Aboriginal primary health care delivery. Professional and dedicated Indigenous Woman CEO’S , Doctors, Clinic Managers, Aboriginal Health Workers , Nurses, Receptionists etc.
IWD is a global day celebrating the social, economic, cultural and political achievements of women.
The theme this year is #PressforProgress, a call to action for accelerating gender equality. Our ACCHO workforce is leading the way.
We can all play a part in improving outcomes for women and this year’s theme provides an opportunity to press even harder for progress in our ACCHO’s
These woman in our tribute today represent the 45 years of ACCHO’s advocating for culturally respectful, needs based approach to improving the health and wellbeing outcomes of our people in the past and now into our healthy futures .
1.NSW : Dr Naomi Mayers one of the founders of Aboriginal Medical Service in Redfern ,AHMRC and NACCHO
2. VIC: Jill Gallagher AO VACCHO CEO 2001-2018
3. QLD : Pamela Mam establishment of the Aboriginal and Islander Community Health Service and Jimbelunga Nursing centre
4. SA : Mary Buckskin (1955 – 2015 ) CEO of AHCSA for 8 years
5.NT : Donna Ah Chee CEO Congress Alice Springs , NACCHO Board Member, Chair AMSANT former CEO NACCHO
6.WA : Vicki O’Donnell. Chair AHCWA : CEO – Kimberley Aboriginal Medical Services.
7.ACT : Julie Tongs OAM CEO Winnunga Nimmityjah Aboriginal Health Service, NACCHO Board Member,
8.TAS. Heather Sculthorpe CEO Tasmanian Aboriginal Centre
1.NSW : Dr Naomi Mayers one of the founders of Aboriginal Medical Service in Redfern ,AHMRC and NACCHO
The University of Sydney recently conferred a Doctor of Letters (honoris causa) upon Naomi Mayers OAM, for her work delivering and transforming Aboriginal and Torres Strait Islander health care
“We’ve come a long way since the Aboriginal Medical Service first opened its doors, thanks to the efforts of so many people,
Of course there remains much work to be done and I urge the younger generations to continue fighting to close the gap in Aboriginal and Torres Strait Islander health outcomes.”
Dr Naomi Mayers in 1972 one of the founders of Aboriginal Medical Service in Redfern and a founding member of the Aboriginal Health and Medical Research Council of NSW and the National Aboriginal and Islander Health Organisation (now NACCHO )
“Australia owes a debt of gratitude to Dr Mayers, for her impressive contribution towards improving health care policy, system delivery and access for Aboriginal and Torres Strait Islander people.
She dedicated her working life to achieving health equity, and the empowerment of her community, in Redfern and beyond.”
Congratulating Dr Mayers, Deputy Vice-Chancellor (Indigenous Strategy and Services) Professor Shane Houston said her work had made a tangible difference to countless people.
An advocate, leader and reformer, Dr Mayers has been at the forefront of change in health service provision to Aboriginal and Torres Strait Islander communities at local, state and national levels for over 40 years.
One of the founders of the first Aboriginal community-controlled health service in Australia in early 1972, the Aboriginal Medical Service in Redfern, Dr Mayers worked as its Administrator, Company Secretary and finally Chief Executive Officer until her recent retirement.
Over 40 years, she guided its transformation from a small shop-front into a nationwide network of services.
Dr Naomi Mayers at the University of Sydney.
A Yorta Yorta/Wiradjuri woman, Dr Mayers was also a founding member of The Sapphires, the all-Aboriginal music group from country Victoria that formed the basis of the popular 2012 film of the same name.
Presented with the honour during a graduation ceremony at the University’s Great Hall, Dr Mayers acknowledged the importance of collaboration and persistence in achieving change.
At the age of 18, Dr Mayers began her work in health as a nurse, at the Royal Women’s Hospital and Royal Children’s Hospital in Melbourne, the Home Hill Hospital in Queensland and St Andrews Hospital in East Melbourne. She was also a board member of the Royal Flying Doctor Service.
She was a founding member of the Aboriginal Health and Medical Research Council of NSW and the National Aboriginal and Islander Health Organisation (NAIHO, now the National Aboriginal Community Controlled Health Organisation); founding president of the Federation for Aboriginal Women; and a member of the first Australian and Torres Strait Islander Commission Regional Council (Metropolitan Sydney).
Dr Naomi Mayers.
She was a witness during the inquiries of the 1977 House of Representatives Standing Committee on Aboriginal Health, and in 1981 she was appointed as a consultant by the Royal Australian College of Ophthalmologists.
Dr Mayers was also Chair of the National Aboriginal Health Strategy Working Party, which authored a pivotal report that introduced innovative Aboriginal health sector reforms which helped shape the 150 Aboriginal Medical Services across Australia today.
She was awarded a Medal of the Order of Australia in 1984 in recognition of her services to the community and holds a doctorate in Aboriginal Affairs from Tranby Aboriginal College in Sydney.
2. VIC: Jill Gallagher AO VACCHO CEO 2001-2018
Update 2018
Jill Gallagher named Victorian Treaty Advancement Commissioner
Ms Gallagher AO, a Gunditjmara woman from Western Victoria who has worked within, led and advocated for the Victorian Aboriginal community all her life, has been named Victorian Treaty Advancement Commissioner.
The Victorian Treaty Advancement Commissioner is a newly created role entrusted with taking the lead in preparing to negotiate the first ever treaty between Aboriginal people and an Australian government
Jill Gallagher AO has never hesitated to seize opportunities to support her community in the pursuit of better health, community autonomy and reclamation of the traditional culture and society of Aboriginal Victorians.
A Gunditjmara woman, Jill was born in the Australian Capital Territory as her parents travelled looking for work. She was 1 of 10 children. Her mother, Frances (nee Winter) grew up at Framlingham in south-west Victoria. Jill’s father, of Irish descent, was accidentally killed when she was a baby.
There were few supports for women, particularly Aboriginal women
Jill spent her childhood in Gippsland, where her mother, like many Victorian Aboriginal people of the era, found seasonal work picking vegetables. This was a time before the emergence of Aboriginal organisations and there were few supports for women, particularly Aboriginal women. The seasonal camps in which the family stayed became their community. An abiding memory for Jill is of a campsite by a river in the evening, dotted with the glow of dozens of campfires.
Jill’s family moved to Collingwood in 1963 when she was eight and her mother found work in a box factory. They had very little. Jill, who had by then attended 19 different primary schools, finished her primary education at George Street Primary School, but only had a short time in secondary education at Fitzroy Girls School. Rebellious and disobedient, she clashed with teachers and left school at the age of 14 to find factory work.
She grasped the opportunity to reclaim knowledge of traditional culture, language, stories and people
In her early twenties, Jill regretted her lack of education. Now with a child of her own, she wanted more from life than factory work and realised that education would help her to support her family.
Jill was fortunate to come across a training scheme for Aboriginal young people, introduced by then Victorian Education Minister Joan Kirner.
She was thrilled to be accepted and began training at the Museum of Victoria. She took advantage of access to the professional development offered there and later took up a position at the Victorian Archaeological Survey.
More importantly, she grasped the opportunity offered by the Museum’s collections to reclaim knowledge of traditional culture, language, stories and people that had been impacted by white settlement and the devastation it left on Aboriginal people.
She saw an opportunity to rediscover truths about Aboriginal society before European settlement and to pass this knowledge on to young people. Jill became a firm advocate of the importance of Aboriginal voices in the collection and management of their heritage, maintaining this passion in a further role as manager of the Heritage Branch of Aboriginal Affairs Victoria.
Jill was and is still is very passionate about the repatriation of Aboriginal cultural property, and the return of ancestors for reburial, being very active in this field since its beginnings in the 1980s.
She worked at the Museum of Victoria when the Aboriginal Legal Service fought to have the Murray Black collection of Aboriginal remains returned to Victoria from institutions such as the University of Melbourne and the National Museum of Australia. Although she moved out of the Aboriginal heritage field in 1998, Jill remained passionate about its importance. For many years she continued to serve on the National Committee for the Repatriation of Skeletal Remains.
Victorian Aboriginal Community Controlled Health Organisation
In 1998 Jill’s commitment to Aboriginal community control saw her take up a position at Victorian Aboriginal Community Controlled Health Organisation (VACCHO), a peak body advocating for the many community controlled Aboriginal health services in Victoria.
Jill was aware that these organisations had been founded to offer meeting places where Aboriginal communities could be visible once again in the landscape. She reinforced VACCHO’s role in supporting its member organisations to stay true to their community beginnings. She also refined and modified their practices to improve health outcomes for Aboriginal Victorians.
Since 2000, VACCHO has offered training for Aboriginal Health Workers via its status as a Registered Training Organisation. Constantly seeking ways to improve health outcomes for Aboriginal Victorians, VACCHO now collects and analyses data collected by its member organisations in order to strengthen their services.
As the CEO of VACCHO since 2001, Jill has seen the organisation grow significantly with current staff numbers at 75. VACCHO has developed innovative preventative and educational health programs, including the Well Person’s Checklist, the Koori Maternity Services Program, and a successful diabetes education initiative.
Strong and effective leadership
One of Jill’s proudest achievements was gaining bipartisan support for the vital ‘Statement of Intent’ signed by the Victorian Premier in August 2008 on behalf of the State government. This statement pledged to close the gap between Indigenous and non-Indigenous Australians in life expectancy, educational achievement and employment opportunities.
In 2010 Jill was inducted to the Victorian Honour Roll of Women. In 2013 she was awarded an Order of Australia in recognition of her strong and effective leadership in Aboriginal health.
She has also been a well-respected member of a number of State government and statutory advisory committees, including the Victorian Early Childhood Development Advisory Committee, the Equal Opportunity Commission Victoria Indigenous Reference Group, the Child Death Review, the Cooperative Research Centre on Aboriginal Health, and the Premiers Aboriginal Advisory Committee.
Jill cites her early career mentors, such as Jim Berg of the Koori Heritage Trust and Terry Garwood of Aboriginal Affairs Victoria, as great influences on her life, inspiring her with the confidence to believe in herself. But most of all she continues to be inspired by her mother’s determination and resilience in the face of everything she endured.
3. QLD : Pamela Mam establishment of the Aboriginal and Islander Community Health Service and Jimbelunga Nursing centre
Pictured here with her family in front of the IUIH building mural 2018
Pamela Mam was born in Richmond in 1938 but came from Palm Island. Her mother was taken from Cook Town during the time of the stolen generation, and was sent away to Palm Island.
Pam’s husbands name is Steve and her children are Tomasina and Mukubi. She has two grandchildren whose names are Darlene and Rendy, with the Ezra families living on Palm Island also.
Pamela started working as a Nurse Aid in Palm Island Hospital and continued to work there for four years. She completed her general training at Townsville Hospital between the years 1954 and 1959. She then went on to Midwifery at the Royal Women’s Hospital.
In 1973 Pamela began work in the Raff Ward of the Royal Children’s Hospital. She was strongly encouraged by her husband to work in a field that would allow her to truly help her people in the area of health. She has been working in this area ever since and this year marks her 55th year in the field. This is a truly remarkable and outstanding feat.
Pamela has said in the past that nursing has at times been a real challenge for her. Though against all the odds and her limited high school education, she has succeeded tremendously in both her personal and her professional life and has forged a career in the difficult and complex world of health.
Being a role model for Indigenous people, and encouraging them to achieve in the way that she has, dispute the challenges, has been a real highlight for Pamela.
Her greatest achievement can be seen in the establishment of the Aboriginal and Islander Community Health Service and Jimbelunga Nursing centre.
4. SA .Mary Buckskin (1958 – 2015 ) CEO of AHCSA for 8 years.
Mary Buckskin (1955 – 2015 ) held the position of CEO for the Aboriginal Health Council of SA Inc (AHCSA) for 8 years. She has nearly 30 years experience in Aboriginal health, working at both state and national level until passing in 2015
Mary had a nursing background with qualifications as a registered nurse, registered midwife holding a Diploma of Nursing and an Advanced Diploma of Community Services Management.
She held a number of different positions throughout her career in Aboriginal health including clinic nurse, community health nurse, senior policy officer, Aboriginal hospital liaison officer and clinical educator.
She was a board member of Nunkuwarrin Yunti Aboriginal Health Service (Adelaide) and past board member of Winnunga Nimmityjah Aboriginal Health Service (ACT) and the Aboriginal Elders and Community Care Services Inc (Adelaide).
5.NT : Donna Ah Chee CEO Congress Alice Springs , Chair AMSANT former CEO NACCHO
Ms Ah Chee is the Chief Executive Officer of the Central Australian Aboriginal Congress Aboriginal Corporation, the Aboriginal community controlled primary health care service in Alice Springs.
Ms Ah Chee is a Bundgalung woman from the far north coast of New South Wales and has lived in Alice Springs for over 25 years.
She has been actively involved in Aboriginal affairs for many years, especially in the area of Aboriginal adult education and Aboriginal health.
In June 2011, Ms Ah Chee moved to Canberra to take up the position of Chief Executive Officer of the National Aboriginal Community Controlled Organisation before returning to Congress in July 2012.
Ms Ah Chee convened the Workforce Working Party under the Northern Territory Aboriginal Health Forum, was Chairperson of the Central Australian Regional Indigenous Health Planning Committee, a member of the Northern Territory Child Protection External Monitoring Committee and jointly headed up the Northern Territory Government’s Alcohol Framework Project Team.
She currently sits on the National Drug and Alcohol Committee and at a local level, represents the Congress on the People’s Alcohol Action Coalition.
In 2016 Associate Professor John Boffa and Ms Donna Ah Chee were recognised by the AMA with its Excellence in Healthcare Award for 2016 for the enormous contribution to reducing harms of alcohol and improving early childhood outcomes for Aboriginal children
See Media Coverage
“This award recognises and acknowledges Professor Boffa and Ms Ah Chee’s unwavering efforts to achieve the best possible health outcomes for Aboriginal people, For almost two decades, they have formed a crucial partnership, working together to implement core services and reform Aboriginal primary health care in the Northern Territory.
They had made a significant contribution to the health of Aboriginal people through their involvement with primary care, research, education and public health.”
Outgoing AMA President, Professor Brian Owler, presented the award at the AMA’s National Conference in Canberra
The Excellence in Health Care Award recognises ongoing commitment to quality health and medical care, policy, and research, and is awarded to an individual or individuals who have made a significant contribution to improving health or healthcare in Australia.
Associate Professor Boffa is the Chief Medical Officer of Public Health at the Central Australian Aboriginal Congress Aboriginal Corporation and has worked in Aboriginal primary care services for more than 25 years.
Ms Ah Chee is the Chief Executive Officer of the Central Australian Aboriginal Congress and is the former CEO of the National Aboriginal Community Controlled Health Organisation.
Professor Owler said the pair had gone above and beyond in their commitment to improving the health of Aboriginal people.
“Professor Boffa and Ms Ah Chee have worked tirelessly together to bring about reforms and accountability in Indigenous Health,” Professor Owler said.
“Their service model on alcohol and drug treatment, which focused on three streams of care including medical, psychological and social and cultural support, resulted in a major alcohol treatment service being funded within an Aboriginal community controlled health service.
“They have initiated major and highly significant reforms in not only addressing alcohol and other drugs, but in collaborating and overcoming many cross cultural sensitivities in working in Aboriginal health care.”
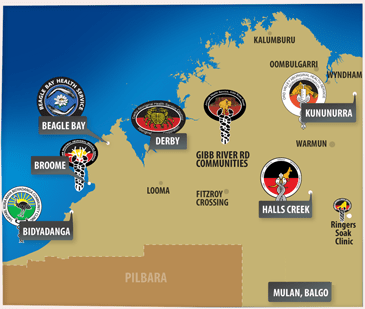
6.WA : Vicki O’Donnell. Chair AHCWA : CEO – Kimberley Aboriginal Medical Services.
Chairperson: Vicki O’Donnell (second from left ) with AHCWA board members Deputy Chairperson: Raymond Christophers Secretary: Fabian Tucker Treasurer: Susan Oakley
I am a Nyikina Mangala Aboriginal woman from Derby where I grew up.
I have worked as a Strategic Leader in Aboriginal Community Controlled Health for the past fifteen years.
This is demonstrated currently in my position of Chief Executive Officer (CEO) for the Kimberley Aboriginal Medical Service (KAMS) in Broome and my previous role as the CEO of the Derby Aboriginal Health Service for 12 years.
KAMS (Kimberley Aboriginal Medical Services Ltd) is a regional Aboriginal Community Controlled Health Service (ACCHS), providing a collective voice and support for a network of member ACCHS from towns and remote communities across the Kimberley region of Western Australia.
KAMS was first established in 1986 as a cooperative between the Broome Regional Aboriginal Medical Service (BRAMS) and the East Kimberley Aboriginal Medical Service (EKAMS) now the Ord Valley Aboriginal Health Service (OVAHS) with membership expanding to Halls Creek health service committee and Fitzroy Crossing community representatives.
These communities saw the benefit of sharing pooled resources and collective effort in the region.
Today, Member services now include;
Broome Regional Aboriginal Medical Service (BRAMS)
Ord Valley Aboriginal Health Service (OVAHS)
Derby Aboriginal Health Service (DAHS)
Yura Yungi Medical Service (YYMS)
Kutjungka Clinical Services (KAMS Remote Clinic)
Beagle Bay Health Services (KAMS Remote Clinic)
Bidyadanga Community (KAMS Remote Clinic)
Nirrumbuk Aboriginal Corporation
KAMS provides a wide range of services including:
Financial and accounting
Regional population health programs
Social and Emotional Well Being Support
Health Promotion
Information Communication Technology Support
Pharmacy support and training
Corporate Services
Accredited health training and education
Research
While the major role is in regional advocacy and support for member services, KAMS also provides comprehensive primary health care services in the remote communities of Beagle Bay, Bidyadanga, Balgo, Mulan and Billiluna.
In 2014 KAMS established Kimberley Renal Services Pty Ltd to manage the provision of regional renal support and dialysis services in Broome, Derby, Kununurra and Fitzroy Crossing.
Summary
My motivation is derived from working in health and specifically Aboriginal Health so that our people can have better access to health, wellbeing and to improved health outcomes in rural, remote and metro areas through Aboriginal Community Controlled Health Services.
My STRENGTHS
1.Advocacy that translates into delivery, and ongoing support of Aboriginal programs across Western Australia at a Regional, State and National level.
2. Extensive expertise and understanding of Aboriginal health.
3.Multiple perspectives of Indigenous issues that results in real health improvement outcomes
7.ACT : Julie Tongs OAM CEOWinnunga Nimmityjah Aboriginal Health Service
Julie Tongs OAM has been the Chief Executive Officer of Winnunga Nimmityjah Aboriginal Health Service since 1998.
Watch Julie on NACCHO TV
Julie has more than 30 years experience working in Aboriginal and Torres Strait Islander affairs and in particular has extensive experience in advising, formulating, implementing and evaluating public health initiatives, programs and policy at a local, regional and national level.
Julie has been a national leader and strong advocate of quality improvement initiatives within the Aboriginal Community Controlled sector.
Julie is the recipient of a number of awards, including the ACT Governor General’s Centenary Medal and the ACT Indigenous Person of the Year. In 2011 Julie received the ACT Local Hero Award within the Australian of the Year Awards 2012, and in 2012 Julie was honoured with the Medal of the Order of Australia.
Julie’s vision is that Winnunga continues to build on its reputation as a national leader in the provision of holistic primary health care services delivered in a culturally appropriate environment that achieves improved health outcomes for Aboriginal and Torres Strait Islander people.
Julie is committed to ensuring that Winnunga offers services that are delivered consistent with best practice standards.
8.Tas. Heather Sculthorpe CEO Tasmanian Aboriginal Centre
Heather has been with the TAC since the early 1970s and despite some time away in Canberra and studying she has stayed with the organisation ever since.
She is the long-term CEO of the TAC, which includes the AHS/ACCHO
In 1982 Heather Sculthorpe became the first Tasmanian Aboriginal to obtain a law degree, from the University of Tasmania
As well as an Arts degree, she has an honours degree in law and a graduate diploma in environmental management and is a Graduate of the Australian Institute of Company Directors.
She has 2 beautiful activist and talented daughters and 2 magnificent granddaughters.
Most of her working life has been as a single parent. She is proud to have assisted the emergence of other Aboriginal women and mothers as staunch advocates for their community.
She considers her most worthy achievements to be quitting smoking after very many years of addiction and having steered the TAC from being a small, community controlled organisation that grew naturally from the big issues of injustice facing the community to a sophisticated multi-million dollar organisation that has survived the tight rope of accountability to its community and to the many competing demands of modern funding and governance requirements.
She remains a firm believer in advanced educational studies for Aboriginal people, a goal that is showing real gains in Tasmania.
And at the same time in Tasmania she sees a real need for community to remain grounded in Aboriginal heritage and culture, a goal that is currently blossoming in Tasmania after so many years of attempts to destroy all cultural memory. She sees this as the way of the future representing a proper holistic approach to Aboriginal primary health care, without which there will be no Aboriginal community in a few generations.
Here is her IWD2018 story in her own words
I’m not into this approach of singling out individual women as role models or heroes or trail blazers.
Everything we do in Aboriginal community services is achieved by the dedicated teams of workers and community pulling in the same direction with the wellbeing of the community as our top priority.
At the Aboriginal Health Service in Tasmania we have role models in so many of our community women now deceased: Ida West, Furley Gardner, Rosalind Atkinson Langford – and those still serving like Annette Peardon, Kerry Sculthorpe, Cheryl Mundy.
In lutruwita/Tasmania it is not customary for us to celebrate achievements of one gender alone.
While women have been at the forefront in Aboriginal community organisations and on committees, it is only by working as one unified community with men, elders and children that we have achieved our major gains.
” We hear so much at this time of year about New Year’s resolutions – eat healthy, quit smoking, get more exercise, drink more water. The list goes on and on and on.
While these are all valid and well intentioned goals, I am urging you to do one simple thing for your health in 2018 which could save your life.
Have your blood pressure checked.
High blood pressure is a key risk factor for stroke and one that can be managed.”
By Stroke Foundation Clinical Council Chair Associate Professor Bruce Campbell see full Press Release Part 1 WEBSITE
” High blood pressure, also referred to as hypertension, is a major risk factor for stroke, coronary heart disease, heart failure, kidney disease, deteriorating vision and peripheral vascular disease leading to leg ulcers and gangrene.
Major risk factors for high blood pressure include increasing age, poor diet (particularly high salt intake), obesity, excessive alcohol consumption, and insufficient physical activity . A number of these risk factors are more prevalent among Indigenous Australians
Based on both measured and self-reported data from the 2012–13 Health Survey, 27% of Indigenous adults had high blood pressure.
Rates increased with age and were higher in remote areas (34%) than non-remote areas (25%).
Twenty per cent of Indigenous adults had current measured high blood pressure.
Of these adults, 21% also reported diagnosed high blood pressure.
Most Indigenous Australians with measured high blood pressure (79%) did not know they had the condition; this proportion was similar among non-Indigenous Australians.
Therefore, there are a number of Indigenous adults with undiagnosed high blood pressure who are unlikely to be receiving appropriate medical advice and treatment.
The proportion of Indigenous adults with measured high blood pressure who did not report a diagnosed condition decreased with age and was higher in non-remote areas (85%) compared with remote areas (65%).
PMC Aboriginal and Torres Strait Islander Health Performance Framework 2014 Report see extracts below PART 2 or in full HERE
Closing the gap in Aboriginal and Torres Strait Islander cardiovascular disease
Cardiovascular disease is the leading cause of death for Aboriginal and Torres Strait Islander people, who experience and die from cardiovascular disease at much higher rates than other Australians.
Aboriginal and Torres Strait Islander people, when compared with other Australians, are:
1.3 times as likely to have cardiovascular disease (1)
three times more likely to have a major coronary event, such as a heart attack (2)
more than twice as likely to die in hospital from coronary heart disease (2)
19 times as likely to die from acute rheumatic fever and chronic rheumatic heart Disease (3)
more likely to smoke, have high blood pressure, be obese, have diabetes and have end-stage renal disease.(3)
“High blood pressure is a silent killer because there are no obvious signs or symptoms, the only way to know is to ask your ACCHO GP for regular check-ups.
Uncontrolled high blood pressure is one of the greatest preventable risk factors that contributes significantly to the cardiovascular disease burden.
The good news is that hypertension can be controlled through lifestyle modification and in more serious cases by blood pressure-lowering medications.”
Part 1 Stroke Foundation Press Release Continued :
A simple step to prevent stroke in 2018
Stroke is a devastating disease that will impact one in six of us. There is one stroke every nine minutes in Australia. Stroke attacks the human control centre – the brain – it happens in an instant and changes lives forever.
In 2018 it’s estimated there will be more than 56,000 strokes across the country. Stroke will kill more women than breast cancer and more men than prostate cancer this year.
But the good news is that it does not need to be this way. Up to 80 percent of strokes are preventable, and research has shown the number of strokes would be practically cut in half (48 percent) if high blood pressure alone was eliminated.
Around 4.1 million of us have high blood pressure and many of us don’t realise it. Unfortunately, high blood pressure has no symptoms. The only way to know if it is a health issue for you is by having it checked by your doctor or local pharmacist.
Make having regular blood pressure checks a priority for 2018. Include a blood pressure check in your next GP visit or trip to the shops. Be aware of your stroke risk and take steps to manage it. Do it for yourself and do it for your family.
If you think you are too young to suffer a stroke, think again. One in three people who has a stroke is of working age.
Health and fitness is big business. But before you fork out big bucks on a personal trainer or diet plan this year, do something simple and have your blood pressure checked.
It will only take five minutes, it’s non-invasive and it could save your life.
Declaration of Interest : Colin Cowell NACCHO Social Media Editor ( A stroke Survivor) was a board member and Chair of Stoke Foundation Consumer Council 2016-17
Part 2PMC Aboriginal and Torres Strait Islander Health Performance Framework 2014 Report or in full HERE
In 2012–13, 10% of Indigenous adults reported they had a diagnosed high blood pressure condition.
Of these, 18% did not have measured high blood pressure and therefore are likely to be managing their condition.
Indigenous males were more likely to have high measured blood pressure (23%) than females (18%).
The survey showed that an additional 36% of Indigenous adults had pre-hypertension (blood pressure between 120/80 and 140/90 mmHg).
This condition is a signal of possibly developing hypertension requiring early intervention. In 2012–13, after adjusting for differences in the age structure of the two populations, Indigenous adults were 1.2 times as likely to have high measured blood pressure as non-Indigenous adults.
For Indigenous Australians, rates started rising at younger ages and the largest gap was in the 35–44 year age group. Analysis of the 2012–13 Health Survey found a number of associations between socio-economic status and measured and/or self-reported high blood pressure.
Indigenous Australians living in the most relatively disadvantaged areas were 1.3 times as likely to have high blood pressure (28%) as those living in the most relatively advantaged areas (22%).
Indigenous Australians reporting having completed schooling to Year 9 or below were 2.1 times as likely to have high blood pressure (38%) as those who completed Year 12 (18%).
Additionally, those with obesity were 2 times as likely to have high blood pressure (37% vs 18%). Those reporting fair/poor health were 1.8 times as likely as those reporting excellent/very good/good health to be have high blood pressure (41% vs 22%).
Those reporting having diabetes were 2.2 times as likely to have high blood pressure (51% vs 23%), as were those reporting having kidney disease (57% vs 26%). One study in selected remote communities found high blood pressure rates 3–8 times the general population (Hoy et al. 2007).
Most diagnosed cases of high blood pressure are managed by GPs or medical specialists. When hospitalisation occurs it is usually due to cardiovascular complications resulting from uncontrolled chronic blood pressure elevation.
During the two years to June 2013, hospitalisation rates for hypertensive disease were 2.4 times as high for Aboriginal and Torres Strait Islander peoples as for non-Indigenous Australians. Among Aboriginal and Torres Strait Islander peoples, hospitalisation rates started rising at younger ages with the greatest difference in the 55–64 year age group.
This suggests that high blood pressure is more severe, occurs earlier, and is not controlled as well for Indigenous Australians.
As a consequence, severe disease requiring acute care in hospital is more common. GP survey data collected from April 2008 to March 2013 suggest that high blood pressure represented 4% of all problems managed by GPs among Indigenous Australians.
After adjusting for differences in the age structure of the two populations, rates for the management of high blood pressure among Indigenous Australians were similar to those for other Australians.
In December 2013, Australian Government-funded Indigenous primary health care organisations provided national Key Performance Indicators data on around 28,000 regular clients with Type 2 diabetes.
In the six months to December 2013, 64% of these clients had their blood pressure assessed and 44% had results in the recommended range (AIHW 2014w).
Implications
The prevalence of measured high blood pressure among Indigenous adults was estimated as 1.2 times as high as for non-Indigenous adults and hospitalisation rates were 2.4 times as high, but high blood pressure accounted for a similar proportion of GP consultations for each population.
This suggests that Indigenous Australians are less likely to have their high blood pressure diagnosed and less likely to have it well controlled given the similar rate of GP visits and higher rate of hospitalisation due to cardiovascular complications.
Research into the effectiveness of quality improvement programmes in Aboriginal and Torres Strait Islander primary health care services has demonstrated that blood pressure control can be improved by a well-coordinated and systematic approach to chronic disease management (McDermott et al. 2004).
Identification and management of hypertension requires access to primary health care with appropriate systems for the identification of Aboriginal and Torres Strait Islander clients and systemic approaches to health assessments and chronic illness management.
The Indigenous Australians’ Health Programme, which commenced 1 July 2014, provides for better chronic disease prevention and management through expanded access to and coordination of comprehensive primary health care.
Initiatives provided through this programme include nationwide tobacco reduction and healthy lifestyle promotion activities, a care coordination and outreach workforce based in Medicare Locals and Aboriginal Community Controlled Health Organisations and GP, specialist and allied health outreach services serving urban, rural and remote communities, all of which can be used to diagnose and assist Indigenous Australians with high blood pressure.
Additionally, the Australian Government provides GP health assessments for Indigenous Australians under the MBS, of which blood pressure measurement is one key element, with follow-on care and incentive payments for improved management, and cheaper medicines through the PBS.
The Australian Government-funded ESSENCE project ‘essential service standards’ articulates what elements of care are necessary to reduce disparity for Indigenous Australians for high blood pressure.
This includes recommendations focusing on primary prevention through risk assessment, awareness and early identification and secondary prevention through medication.
Wednesday by 4.30 pm for publication each Thursday
1.1 NACCHO CEO Pat Turner to build on the success of Aboriginal Community Control Health Services
Pat Turner has been appointed for a further three years until July 2020 by the National Aboriginal Community Controlled Health Organisation (NACCHO) Board.
NACCHO Deputy Chairperson, Sandy Davis welcomed Ms Turner’s appointment highlighting her extensive life experiences in Aboriginal affairs, government, academia and corporate practice.
Sandy also ‘acknowledged her invaluable record of public service achievements and that her leadership style comes at an important time for NACCHO with new governance arrangements to be discussed with members’ at our Annual General Meeting in Canberra in November.
Pat will help create real, meaningful and lasting change for NACCHO that will strengthen community control and keep Aboriginal health in Aboriginal hands’ he said.
Pat recently finalised a new network funding agreement for supporting community controlled Aboriginal health service with the Commonwealth. This will allow for better, more targeted investment in efforts to close the health gap for Aboriginal people. Pat has consistently said that ‘governments at all levels must do more to join the dots between education, housing, employment and other social determinants if we are to significantly improve health outcomes for our people and Close the Gap they have spoken about for the best part of a decade.’
Pat has been delivering on the Board’s agenda to consult with members to update our NACCHO Constitution and she has spent the last few months criss-crossing Australia to obtain the views and opinions of our Members and Affiliates about NACCHO constitutional changes.
She will continue to work on strengthening and expanding the Aboriginal Community Controlled Health Sector, maintaining its strategic directions, cutting unnecessary red tape and building a closer relationship between all our organisations. ‘We want to build on the success of community control in improving health outcomes for our people’ she said.
Pat is of Arrernte and Gurdanji descent and was awarded the Order of Australia (AM) in 1990 for her contribution to public service.
1.2 National : 2017 NACCHO Members’ Conference and AGM Registrations : Only 28 days to go
On Tuesday 2 October there was only 28 days to go and due to high demand the conference AGM is nearly booked out
This is an opportunity to show case grass roots best practice at the Aboriginal Community Controlled service delivery level.
In doing so honouring the theme of this year’s NACCHO Members’ Conference ‘Our Health Counts: Yesterday, Today and Tomorrow’.
These girls and boys are representing the Healthy Lifestyle Values and doing us proud today! Well done everyone on being deadly team players and making healthy choices!
Check out their other healthy lifestyle tips below. HERE
3.NSW : In the Shoalhaven region Aboriginal Health is everyone’s business
Illawarra Shoalhaven Local Health District (ISLHD) has joined local Aboriginal Community Controlled Health Services, the Primary Health Network and the University of Wollongong in committing to work together to bring about positive changes to Close the Gap on health inequalities for our Aboriginal communities.
A partnership agreement was formally signed on Friday by leaders of the South Coast Aboriginal Medical Service; Oolong House – Drug and Alcohol Rehabilitation Centre; Illawarra Aboriginal Medical Service; Waminda South Coast Women’s Health and Welfare Aboriginal Corporation; University of Wollongong; COORDINARE – South Eastern NSW Primary Health Network; and Illawarra Shoalhaven Local Health District.
A special ceremony, including a corroboree, smoking ceremony and performances by the Doonooch Dancers led by Joe Brown-McLeod and Larry McLeod,
and a stirring welcome to country by Uncle Tom Moore preceded the official signing of the agreement.
ISLHD Chief Executive Margot Mains said the agreement aims to support, promote and strengthen the existing local relationships and strong ties that have been developed over many years.
“The signing of the partnership agreement marks a new beginning for our journey in working collaboratively to close the health and life expectancy gap between Aboriginal people and non-Aboriginal Australians,” Ms Mains said.
4.NT : Ken Wyatt opens our NACCHO #OchreDay2017 summit in Darwin
Losing his nephew to the same preventable disease that afflicts so many Aboriginal Australians galvanised Ken Wyatt to make indigenous men’s health a “top priority” of his political agenda.
The Federal Indigenous Health Minister says his nephew was a promising musician but died in June, aged just 35, after a battle with diabetes and chronic renal and heart disease.
“One of Jason’s killers was kidney failure, the same devastating condition that claimed the life of beloved musician, Dr G Yunipingu,” Mr Wyatt told a national men’s health conference in Darwin.
“His close family and friends are now working on a media project to fulfil his dying wishes – to get the word out to indigenous men in particular, to take their health seriously, to own it.”
Aboriginal men have the poorest health of any group within the Australian population, which Mr Wyatt says is “nothing short of a national tragedy”.
They suffer kidney health problems at five times the rate of their non-indigenous counterparts, and are dying more than 10 years younger.
Winner of the Jaydons Adams Award
From the left, Mr Mark and Mrs Lizzie Adams with Nathan Cubillo-Jones and AMSANT CEO John Paterson
He’s just graduated this year from his studies as an Indigenous health practitioner and in between playing local Aussie rules and Rugby league, he worked tirelessly with Danila Dilba health service and has recently been appointed manager of the new Malak clinic.
5. QLD : Inquiry into service delivery in remote and discrete Aboriginal and Torres Strait Islander communities : Draft report consultation
The draft report is scheduled to be released in early October 2017.
We are seeking your comments and views on the draft report, and will be undertaking further consultation during October and early November.
The Commissioner Bronwyn Fredericks will be briefing and consulting with stakeholders in the following locations:
9 October 2017 (1pm to 3pm) – Cairns, Doubletree Hilton Hotel
10 October 2017 – Yarrabah
11 October 2017 – Kowanyama
12 October 2017 – Lockhart River
13 October 2017 – Aurukun
16 October 2017 – Gladstone (LGAQ conference)
17 October 2017 – Woorabinda
20 October 2017 – Brisbane
Further consultations will be scheduled in the coming weeks at Mt Isa, Mornington Island, and Thursday Island – details will be published on the QPC website as they become available.
Consultations will include round tables in Cairns, Mt Isa, Thursday Island and Brisbane.
Please register your interest to attend a consultation or round table here.
If you would like to meet with the Commissioner or the inquiry team either as part of the consultation rounds or via teleconference, please contact us on (07) 3015 5111 or enquiry@qpc.qld.gov.au
6.ACT : NACCHO/WinnungaNimmityjah Aboriginal Health Service mental health webinar in conjunction with the Mental Health Professionals Network
On Wednesday the 13th of September 2017, NACCHO facilitated a mental health webinar in conjunction with the Mental Health Professionals Network as part of its professional development work.
This mental health webinar focused on reducing the mental health impacts of indigenous incarceration on people, communities and services.
The discussion was conducted by an Indigenous interdisciplinary panel (see below for further details). A post-discussion Q&A was also conducted between the panel and guests, recordings of which can be accessed below.
THE PANEL
Julie Tongs OAM (CEO Winnunga Nimmityjah Aboriginal Health Service)
Dr Louis Peachey (Rural Generalist)
Dr Marshall Watson (Psychiatrist)
Dr Jeff Nelson (Psychologist)
Facilitator: Dr Mary Emeleus (General Practitioner and Psychotherapist).
7.WA : Puntukurnu Aboriginal Medical Service’s Tackling Indigenous Smoking team to create Anti Smoking Ads
The project, organised by Puntukurnu Aboriginal Medical Service’s Tackling Indigenous Smoking team, will be carried out with funding from a Healthway Indigenous Health Promotion grant and the Federal Government’s Tackling Indigenous Smoking Program.
Puntukurnu Aboriginal Medical Service regional tobacco coordinator Danika Tager said smoking rates in the East Pilbara were exceptionally high and more needed to be done to support communities to address tobacco addiction.
Filmmakers will work with youth in four remote Aboriginal communities in the East Pilbara to shed light on the personal stories of local smokers and warn about the perils of the deadly habit.
Young people, assisted by a professional production team, will create a series of short films as part of the “you CAN quit” project, to document the stories of community members who have successfully kicked the habit and those who have been affected by smoking-related illnesses in Jigalong, Parnngurr, Punmu and Kunawarritji.
Statistics from the Federal Department of Health show that tobacco smoking is responsible for one in five Aboriginal and Torres Strait Islander deaths, with the number substantially higher in remote areas.
“Smoking rates in remote East Pilbara communities are as high as 80% and tobacco use is the single most preventable cause of death and disease in this population,” Ms Tager said.
“Through this important film project we hope to encourage people in these communities to quit smoking, as well as air the many benefits of quitting and where they can find help and support.”
Filming of the four short films will start September 19. It is expected the films will be screened in each community on completion and also be aired on indigenous television stations and social media.
Ms Tager said the project was unique in that the films would be entirely community owned and directed, giving young people the opportunity to actively make a difference in their community.
“Youth will be responsible for all aspects of researching, shooting, editing and promoting the films” she said.
“All too often NGOs will come into a community with a health message that may or may not be relevant, and expect it to change people’s behaviour,” she said.
“What we are doing here is empowering the community to send its own messages and fight tobacco-related harm using its own experience and stories.”
The project will also involve a series of posters to celebrate non-smokers in the communities, and offer education sessions and details about the availability of support programs.
The Puntukurnu Aboriginal Medical Service (PAMS) is a community controlled health organisation that provides primary health care, 24-hour emergency services and preventative health and education programs in the communities of Jigalong, Parnngurr, Punmu and Kunawarritji.
8. Tas : Tasmanian Aboriginal Centre to celebrate our communities journey of breast cancer & raise awareness
Please join us at piyura kitina (Risdon Cove) on Thursday, 12th October at 1.30pm, to celebrate our communities journey of breast cancer & raise awareness of this disease.
Afternoon tea, will be provided, please contact Emma on
6234 0777 or Freecall 1800 132 260 if you require transport.
9.SA : Aboriginal Health Council of SA and South Australian Aboriginal Chronic Disease Consortium
The South Australian Aboriginal Chronic Disease Consortium (the Consortium) was launched on 18 May 2017, as a collaborative partnership formed between the South Australian Aboriginal Health Partnership (comprising of SA Health, Aboriginal Health Council of SA and Department of Health – Commonwealth) and the South Australian Academic Health Science and Translation Centre.The Translation Centre represents a partnership between SA Health, South Australian Health and Medical Research Institute (SAHMRI), University of Adelaide, Flinders University, University of South Australia, Aboriginal Health Council of South Australia, Health Consumers Alliance of South Australia, Adelaide Primary Health Network, Country SA Primary Health Network and Cancer Council SA. The Translation Centre has 9 priority areas of which one is Aboriginal Health.
Consortium Vision
The Consortium’s vision is to reduce the impact of chronic disease experienced by Aboriginal and Torres Strait Islander people living in South Australia through the successful implementation of the priorities identified within 3 plans: The South Australian Aboriginal Cancer Control Plan 2016-2021, the South Australian Aboriginal Heart and Stroke Plan 2017-2021 and the South Australian Aboriginal Diabetes Strategy 2017-2021.How will the Consortium Work
The responsibility to oversee the implementation activity of the SA Aboriginal Chronic Disease Consortium rests within its governance structures. The Consortium has 5 active working groups including an Executive Group, an Aboriginal Community Reference Group and three condition-specific leadership groups representing Diabetes, Cancer and Heart and Stroke. We refer to the people and organisations on these groups as our members.
Who is working in the Consortium Coordinating Centre?
The team comprises of two full time staff. Wendy Keech is the Senior Research Translation Manager and Executive Officer. Wendy is supported by Douglas VJ Clinch, in a Project Officer role overseeing and supporting the various governance groups of the Consortium. Strategic policy and cultural advice and support is being provided by Kim Morey and Neville Fazulla both on a part-time basis to the team, and have particular focus on supporting the community reference group. Andrea McKivett, has been providing her clinical, technical and cultural support to the team since the inception of the Consortium, with Katharine McBride recently joining the team to provide technical support one day a week. The team come from various backgrounds and disciplines required to support the work of the Consortium, and all are passionate people with a strong commitment to making a difference to the health and wellbeing of Aboriginal people in South Australia.
If you would like any further information please don’t hesitate to contact Wendy Keech, on (08) 81284228, email: wendy.keech@sahmri.com or Doug VJ Clinch, on (08) 81284893 or email: douglas.clinch@sahmri.com.
” It is critical that responses to support a young person’s mental health be culturally sensitive and gender sensitive and that they address the structural issues that contribute to higher levels of psychological distress for young females and for Aboriginal and Torres Strait Islander young people.
For example, we know that Aboriginal and Torres Strait Islander people continue to be adversely affected by racism, disconnection from culture, and the long history of dispossession. All of these factors contribute to poor mental health, substance misuse and higher suicide rates.
As a matter of priority, suicide prevention programs that are tailored to the needs of the whole community and focussed on prevention should be available to Aboriginal and Torres Strait Islander people. All programs should be offered in close proximity to community and should be age appropriate as well as culturally sensitive.”
Download a copy of the Five-Year Youth Mental Health Report
Ref 2 :Download the Draft Fifth National Mental Health Plan at the link below:
“The release of the Draft Fifth National Mental Health Plan is another important opportunity to support reform, and it’s now up to the mental health sector including consumers and carers, to help develop a plan that will benefit all.”
A successful plan should help overcome the lack of coordination and the fragmentation between layers of government that have held back our efforts to date.”
NACCHO and Mental Health Australia CEO Frank Quinlan have welcomed the release of the Draft Fifth National Mental Health Plan and is encouraging all ACCHO stakeholders to engage with the plan during the upcoming consultation period.
Download the Draft Fifth National Mental Health Plan at the link below:
“Clearly Australia’s mental health system is failing Aboriginal people, with Aboriginal communities devastated by high rates of suicide and poorer mental health outcomes.
Poor mental health in Aboriginal communities often stems from historic dispossession, racism and a poor sense of connection to self and community. It is compounded by people’s lack of access to meaningful and ongoing education and employment. Drug and alcohol related conditions are also commonly identified in persons with poor mental health.
While there was no quick fix for the crisis, an integrated strategy led by Aboriginal community controlled health services is a good starting point.
The National Mental Health Commission Review recommended the establishment of mental health and social and emotional wellbeing teams in Aboriginal Community Controlled Health Services, linked to Aboriginal and Torres Strait Islander specialist mental health services.
None of these can be fixed overnight but we can’t ignore the problems. We are on the brink of losing another generation of Aboriginal people to suicide, poor health and substance abuse.”
What we do know is the solution must be driven by Aboriginal leaders and communities – a model that is reaping great rewards in the Aboriginal Community Controlled health sector.
It must be a community based approach, backed up by governments of all levels.”
NACCHO Chairperson, Matthew Cooke
Ref 4 :Extra info provided by Tom Calma
Prof Pat Dudgeon and Tom Calma chair the ATSI Mental Health and Suicide Prevention Advisory Group to the Commonwealth and Pat Chairs NATSIMHL, the group who created the Gayaa Dhuwi.
Bottom line is that the community should feel confident that all the major initiatives in mental health and suicide prevention are being lead by our people and more can be found at http://natsilmh.org.au
Action urgently needed to stem rising youth mental illness
Last week Mission Australia released its joint Five-Year Youth Mental Health Report with Black Dog Institute, sharing the insights gathered about the mental health of Australia’s young people during the years 2012 to 2016.
Learning what young people think is so important to the work we do at Mission Australia. By checking in with them we discover their thoughts about their lives and their futures, and what concerns them most.
The Five Year Mental Health Youth Report presents the findings of the past five years on the rates of psychological distress experienced by young Australians, aged 15-19.
Almost one in four young people met the criteria for having a probable serious mental illness – a significant increase over the past five years (rising from 18.7% in 2012 to 22.8% in 2016).
Across the five years, females were twice as likely as males to meet the criteria for having a probable serious mental illness. The increase has been much more marked among females (from 22.5% in 2012 to 28.6% in 2016, compared to a rise from 12.7% to 14.1% for males).
Young people with a probable serious mental illness reported they would go to friends, parents and the internet as their top three sources of help. This is compared to friends, parents and relatives/family friends for those without a probable serious mental illness.
In 2016, over three in ten (31.6%) of Aboriginal and Torres Strait Islander respondents met the criteria for probable serious mental illness, compared to 22.2% for non-Indigenous youth.
In light of these findings, Catherine Yeomans, Mission Australia’s CEO said: “Adolescence comes with its own set of challenges for young people. But we are talking about an alarming number of young people facing serious mental illness; often in silence and without accessing the help they need.
The effects of mental illness at such a young age can be debilitating and incredibly harmful to an individual’s quality of life, academic achievement, and social participation both in the short term and long term.
Ms Yeomans said she was concerned that the mental health of the younger generation may continue to deteriorate without extra support and resources, including investment in more universal, evidence-based mental health programs in schools and greater community acceptance.
Given these concerning findings, I urge governments to consider how they can make a major investment in supporting youth mental health to reduce these alarming figures, Ms Yeomans said.
“We need to ensure young people have the resources they need to manage mental health difficulties, whether it is for themselves or for their peers. Parents, schools and community all play a vital role and we must fully equip them with the knowledge and skills to provide effective support to young people.”
The top issues of concern for those with a probable serious mental illness were: coping with stress; school and study problems; and depression. There was also a notably high level of concern about other issues including family conflict, suicide and bullying/emotional abuse.
The report’s finding that young people with mental illness are turning to the internet as a source of help with important issues also points to prevailing stigma, according to Black Dog Institute Director, Professor Helen Christensen.
“This report shows that young people who need help are seeking it reluctantly, with a fear of being judged continuing to inhibit help-seeking,” said Professor Christensen.
“Yet evidence-based prevention and early intervention programs are vital in reducing the risk of an adolescent developing a serious and debilitating mental illness in their lifetime. We need to take urgent action to turn this rising tide of mental illness.
“We know that young people are turning to the internet for answers and our research at Black Dog Institute clearly indicates that self-guided, online psychological therapy can be effective in reducing symptoms of depression and anxiety.
“While technology can be a lifeline, e-mental health interventions must be evidence-based and tailored to support young people’s individual needs. More investment is needed to drive a proactive and united approach to delivering new mental health programs which resonate with young people, and to better integrate these initiatives across schools and the health system to help young people on a path to a mentally healthier future.”
Armed with this information we are able to advocate on their behalf for the support services they need, and for the broader policy changes.
The Five-Year Youth Mental Health Report shows some alarming results with almost one in four young people meeting the criteria for a probable serious mental illness (PSMI). That figure has gone up from 18.7 per cent in 2012 to 22.8 per cent in 2016.
Girls were twice as likely as boys to meet the criteria for having a PSMI, and this figure rose from 22.5% in 2012 to 28.6% in 2016, compared to a rise from 12.7% to 14.1% for boys.
An even higher number of Aboriginal and Torres Strait Islander respondents met the criteria for having a probable serious mental illness (PSMI ) at 31%.
These results make it clear that mental illness is one of the most pressing issues in our communities, especially for young people, and one that has to be tackled by the governments, health services, schools and families.
Three quarters of all lifetime mental health disorders emerge by the age of 24, but access to mental health services for this age group is among the poorest, with the biggest barriers being community awareness, access and acceptability of services.
What we need is greater investment in mental health services that are tailored to the concerns and help seeking strategies of young people and are part of a holistic wrap around approach to their diverse needs.
For young women, we know that a large proportion (64%) were extremely or very concerned about body image compared to a far smaller number of males (34.8%).
Such a finding suggests that social pressures such as discrimination based on ideals of appearance may need to be addressed to tackle this gender disparity in the levels of probable serious mental illness among girls.
And although girls are more likely to be affected negatively by body image issues, they are more likely to seek help when they need it than boys.
Clearly then, and for a variety of reasons, an awareness of gendered differences is a crucial component in the management of mental health issues.
We need to ensure that all young people, whether they live in urban areas or regional, have the resources they need to manage mental health difficulties, whether it is for themselves or for their peers. Parents, schools and community all play a vital role and we must fully equip them with the evidence-based knowledge and skills to provide effective support to young people.
” Little J, he’s five and Big Cuz, she’s nine. They’re a couple of Indigenous Australian kids living with their Nanna and Old Dog. Little J and Big Cuz are busy with the ups and downs of playground and classroom.
There’s always something surprising going on whether it’s at school, in the backyard… or beyond. The gaps in Nanna’s ramshackle fence lead to Saltwater, Desert and Freshwater Country.
With the help of Nanna and their teacher Ms Chen, Little J and Big Cuz are finding out all about culture, community and country
We hope that by providing children with a window into the often-mysterious world of school we can achieve our aim of successful school transition for Indigenous preschool children, a transition that prepares them for a thrilling, lifelong learning journey.”
Little J and Big Cuz animated series starts Easter 2017
“You will also note the reference to ‘whole child development’ in the model. By this we mean that children need to grow not only academically but emotionally, socially, physiologically, and culturally
Strong relationships between schools, families, and community agencies (in health, children’s services, etc.) are therefore critically important. In order for children to learn, they need to be safe, nourished, stimulated, engaged, and ideally confident.”
Tony Dreise (pronounced ‘drice’) descends from the Guumilroi people of north-west New South Wales and south-west Queensland. He was a Principal Research Fellow and Hub Leader for Indigenous Education at the Australian Council for Educational Research (ACER). See Article Below
The first episode of Little J & Big Cuz, the ground-breaking new animated television series aimed at supporting a successful transition from home to school for Indigenous children, is set to premiere on NITV at 7.30pm AEST on Friday 28 April.As previously reported, the series follows lead characters Little J (voiced by Miranda Tapsell) and Big Cuz (Deborah Mailman) as they explore their world and discover more about their culture and the great things that school has to offer.To coincide with the series broadcast, a new Little J & Big Cuz website will also be launched, containing games for children, supporting resources for families and educational resources for teachers.For further updates about Little J & Big Cuz please visit www.littlejandbigcuz.com.au and join the mailing list.These educational resources have been developed by ACER with Indigenous Education Consultants Dr Sue Atkinson, Jess Holland, Elizabeth Jackson-Barrett, Priscilla Reid-Loynes and Alison Wunungmurra, along with former ACARA Senior Education Officer Deborah Cohen and with support from Dr Mayrah Driese in the role of critical friend.
Little J and Big Cuz; a 13 x 13 minute animated series ( see each episode below ) follows the adventures of five-year-old Little J and his older cousin Big Cuz, who live with their Nanna and whose outback life and adventures at home and school form the basis of each episode.
The series was previewed in the Northern Territory 2016 when SBS showcased the series to delegates at the Remote Indigenous Media Festival at Yirrkala in North East Arnhem Land.
Little J and Big Cuz is in production for NITV by Ned Lander Media. The ACTF will distribute the series, with production investment from ACER, Screen Australia, Film Victoria and Screen Tasmania.
Much of the story telling will be visual or carried by the narrator, making it easier to re-voice the show into multiple Indigenous languages.
The intention is that community members will be engaged and funded to re-voice the series.
The production will assist in setting up this process. It is also intended that children whose first language is not English will watch it in both English and their own language at home and school.
Episodes
Episode 1 – Lucky Undies:
Little J’s new undies have special powers – so how can he play basketball without them?
Episode 2 – Wombat Rex:
Big Cuz tricks Little J into believing that the Giant Wombat is not extinct.
Episode 3 – New Tricks:
Little J frets that his dream of being an acrobat is not the RIGHT dream…
Episode 4 – Right Under Your Nose:
On their quest to the beach, Little J, Nanna and Big Cuz struggle to find what they need before sunset.
Episode 5 – Goanna Ate My Homework”
Little J gets confused hunting bush tucker when he follows his own tracks.
Episode 6 – Big Plans:
When the “big kids” won’t play with him, Little J creates a tantalizing adventure – in the back yard.
Episode 7 – Hopalong:
When B Boy comes to stay, Little J is miffed – until they work together caring for an injured baby kangaroo.
Episode 8 – Where’s Aaron?
Aaron the class mascot is missing…and Little J fears he’s lost in the desert.
Episode 9 – Old Monster Dog:
Little J is convinced there’s a real live monster in the backyard.
Episode 10 – Transformation:
Can Big Cuz face dancing in front of the school, and will Little J ever see his caterpillar again?
Episode 11 – Nothing Scares Me:
Little J knows there’s something that scares him but he’s even more scared of being found out.
Episode 12 – Territories:
Big Cuz and Little J must put aside their differences to outwit a territorial magpie.
Episode 13 – Night Owl & Morning Maggie:
Fascinated by an owl in the backyard, Little J turns nocturnal with disastrous results.
School Readiness Initiative: Little J & Big Cuz
ACER and partners have assembled a cast of expert players to meet the exciting challenges posed by the School Readiness Initiative: Little J & Big Cuz
Little J & Big Cuz
The School Readiness Initiative includes a television series that has been developed and is now being realised by experienced producer Ned Lander, with partners NITV, Screen Australia, Film Victoria, Screen Tasmania, ACER and the Australian Children’s Television Foundation.
The TV show is a fun, animated series constructed as a narrative.
The educational foundations are implicit rather than explicit – school is simply a part of life. Episodes depict school life and include activities that occur in this space, such as show-and-tell, lunchtime, school performances and so on. Children viewing the show will follow lead character, Little J, on his adventures as he comes to understand and enjoy the sometimes unfamiliar environment that can be school, and the greater world around him.
The animated nature of the series allows re-voicing in Indigenous languages. A small number of major languages will be re-voiced in the first year with further language versions produced in association with the communities interested in doing this.
In addition, ACER is working with Indigenous Education consultant Priscilla Reid-Loynes to develop innovative educator resources to support the series. The materials being developed integrate with the series around episode themes and stories, and can be used by educators within and outside of the classroom.
These resources will be tailored to work within preschools and schools and will have a foundation in the Early Years Learning Framework and the National Curriculum.
Ready children, ready schools
Being school ready includes the development of foundational literacy and numeracy skills, engagement in learning, and positive attitudes towards education and school.
Of equal importance for students and their families is an understanding of how school works, what is expected of them and what they should expect from school.
The initiative is not just focussed on the child being ready for school, but the school also being ready for the child. ‘Ready schools’ value the skills that Indigenous children bring, they acknowledge families as the first teachers and recognise the role that families and communities play in supporting lifelong development.
Evaluating our effectiveness
The Dusseldorp Forum is providing support for the important task of evaluating the impact of the initiative for children, communities and schools. Results from the evaluation will assist in developing future series and will help to tailor resources in order to maximise the overall effectiveness of the initiative.
We hope that by providing children with a window into the often-mysterious world of school we can achieve our aim of successful school transition for Indigenous preschool children, a transition that prepares them for a thrilling, lifelong learning journey.
ACER is still looking for partners to support the development of resources for educators and outreach materials for families and communities. Please contact Lisa Norris to express your interest +61 3 9277 5520.
School transition made easier with the help of Little J and Big Cuz
A new television series seeks to support the successful transition from home to school for Indigenous children and their families.
‘This article first appeared in Teacher, published by ACER. Reproduced with kind permission. Visit www.teachermagazine.com.au for more.’
Improving Indigenous attendance – the role of teachers
Tony Dreise (pronounced ‘drice’) descends from the Guumilroi people of north-west New South Wales and south-west Queensland. He was a Principal Research Fellow and Hub Leader for Indigenous Education at the Australian Council for Educational Research (ACER). Tony holds a Bachelor of Teaching degree and a Masters of Public Administration with the Australia and New Zealand School of Government. He is undertaking his PhD at ANU, where he is exploring the relationship between Australian philanthropy and Indigenous education. He has over 20 years professional experience in public policy, research, education, and Indigenous affairs.
Recently I co-authored a paper on Indigenous school attendance. In our paper, we found that school attendance among Indigenous children and young people has been improving over recent decades and years.
There is still a way to go – latest data indicate a 10 per cent attendance gap between Indigenous and non-Indigenous students. In some parts of Australia, it is much larger at near 30 per cent. We found that regular school attendance is particularly challenging for Indigenous students in remote areas and in secondary schooling.
To turn this around, we argue that expectations need to be ‘really high’ and ‘highly real’. By that we mean: ‘…‘really high’ expectations of schools, students and parents and carers, and ‘highly real’ expectations about the social and economic policies and environments that stymie educational success.’
Educational research throughout the world points to the importance of school cultures that are driven by ‘high expectations’ of teachers and students alike. Within these school cultures, principals are leading, teachers are teaching smart and students are working hard.
A ‘catch 22’ dilemma
Our paper also contends that the relationship between education and wellbeing is akin to a ‘catch 22’ dilemma. That is, we know that education is key to turning around current levels of Indigenous socioeconomic disadvantage. In other words, education is an investment not a cost.
In a paper called Education and Indigenous Wellbeing (Australian Bureau of Statistics, 2011), the ABS presents a compelling relationship between education and social wellbeing among Aboriginal and Torres Strait Islander people. In addition to improving employment prospects, ABS data show that Indigenous people with education qualifications are more likely to own a home or be paying off a mortgage, less likely to live in overcrowded housing, less likely to be arrested, less likely to smoke or misuse alcohol, and more likely to enjoy greater overall wellbeing.
We also know that the current state of poverty and dysfunction that communities find themselves in adversely impacts on young people’s academic growth. Children find it hard to learn on empty stomachs for example. Teenagers will find it difficult to attend school if they’re being bullied at school because of their race. Hence the ‘catch 22’ dilemma.
So how do we turn around rates of school attendance in locations where it is poor? And more specifically, what can teachers do?
Demand and supply
In our paper, we present the following diagram which represents the need for balance between ‘demand’ and ‘supply’ factors in education:
[Graphic from ‘Indigenous school attendance: Creating expectations that are ‘really high’ and ‘highly real’]
In fashioning responses to current educational inequities, school systems and policymakers tend to favour ‘supply’ side levers such as spending more on professional development among teachers, or employing more Indigenous education assistants, or allocating more to information technology. These are all important, but we cannot afford to overlook the equally important job of attending to the demand side of the education. That is, investing in communities to foster a love of lifelong learning and demand for quality teaching and learner responsiveness. It also means that teachers and schools are delivering quality teaching through culturally-customised, learner-centred and strengths-based approaches. It also means fostering bonds and affinity between teachers and students. Relationships of trust are of paramount importance.
You will also note the reference to ‘whole child development’ in the model. By this we mean that children need to grow not only academically but emotionally, socially, physiologically, and culturally. Strong relationships between schools, families, and community agencies (in health, children’s services, etc.) are therefore critically important. In order for children to learn, they need to be safe, nourished, stimulated, engaged, and ideally confident.
What can teachers do?
Teachers can do a number of practical things to meet the needs of the ‘whole child’. One is the delivery of a full and rich curriculum, whereby learners are engaging in literacy and numeracy, bi-cultural and social growth, music, arts, science, and physical education. Where the purpose and objectives of lessons are clearly understood by learners, and the methods of teaching are energetic and diverse – from teacher-led, to peer-led, to project-driven, to ICT-based, and community- (excursion) based; depending upon what needs to be learnt.
Second, creating school cultures whereby Indigenous cultures and peoples are respected, by consistently engaging the families of learners, not just during NAIDOC week. Where teachers and school leaders are fostering genuine interest in the child’s life, be it their sporting life, their cultural life, their social and family life. Third, by searching and building upon learners’ strengths. Fourth, by adopting ‘growth mindsets’, so that teaching is constantly oriented toward personal improvement, daily, weekly, yearly – which means assessing for growth that goes beyond mere ‘pass/fail’ thinking.
Teachers can also work with their school and community leaders in bringing about initiatives that actively tackle forces that stymie student flourishing. The little things can make a big difference. For example, Brekkie Clubs can literally provide food for thought. Storing spare stationery and school uniforms in a cupboard can help overcome a sense of shame among students whose family circumstances may be rocky.
School leaders and teachers can foster a culture of ‘school matters’ by data collecting, rewarding regular attendance and building bridges between homes and school. Schools can also think of themselves as ‘hubs’ for child development and growth, by integrating children’s academic growth with their health, wellbeing and safety by working with government and community non-government agencies.
Finally, school and community leaders can work together to ensure that Indigenous learners gain access to the services that they require, be it speech pathology, psychological counselling, literacy and numeracy coaching, or culturally affirming student support services.
” Merri’s story is not uncommon. Studies show that women with physical, sensory, intellectual, or psychosocial disabilities (mental health conditions) experience higher rates of domestic and sexual violence and abuse than other women.
More than 70 per cent of women with disabilities in Australia have experienced sexual violence, and they are 40 per cent more likely to face domestic violence than other women.
Indigenous women are 35 times more likely to be hospitalised as a result of domestic violence than non-Indigenous women. Indigenous women who have a disability face intersecting forms of discrimination because of their gender, disability, and ethnicity that leave them at even greater risk of experiencing violence — and of being involved in violence and imprisoned
” In-prison programs fail to address the disadvantage that many Aboriginal and Torres Strait Islander prisoners face, such as addiction, intergenerational and historical traumas, grief and loss. Programs have long waiting lists, and exclude those who spend many months on remand or serve short sentences – as Aboriginal and Torres Strait Islander people often do.
Instead, evidence shows that prison worsens mental health and wellbeing, damages relationships and families, and generates stigma which reduces employment and housing opportunities .
To prevent post-release deaths, diversion from prison to alcohol and drug rehabilitation is recommended, which has proven more cost-effective and beneficial than prison , International evidence also recommends preparing families for the post-prison release phase. ‘
Dying to be free: Where is the focus on the deaths occurring post-prison release? Article 1 Below
Article from Page 17 NACCHO Aboriginal Health Newspaper out Wednesday 16 November , 24 Page lift out Koori Mail : or download
As the world celebrates International Women’s Day, this week I think of ‘Merri’, one of the most formidable and resilient women I have ever met.
A 50-year-old Aboriginal woman with a mental health condition, Merri grew up in a remote community in the Kimberley region of Western Australia. When I met her, Merri was in pre-trial detention in an Australian prison.
It was the first time she had been to prison and it was clear she was still reeling from trauma. But she was also defiant.
“Six months ago, I got sick of being bashed so I killed him,” she said. “I spent five years with him [my partner], being bashed. He gave me a freaking [sexually transmitted] disease. Now I have to suffer [in prison].”
I recently traveled through Western Australia, visiting prisons, and I heard story after story of Indigenous women with disabilities whose lives had been cycles of abuse and imprisonment, without effective help.
For many women who need help, support services are simply not available. They may be too far away, hard to find, or not culturally sensitive or accessible to women.
The result is that Australia’s prisons are disproportionately full of Indigenous women with disabilities, who are also more likely to be incarcerated for minor offenses.
For numerous women like Merri in many parts of the country, prisons have become a default accommodation and support option due to a dearth of appropriate community-based services. As with countless women with disabilities, Merri’s disability was not identified until she reached prison. She had not received any support services in the community.
Merri has single-handedly raised her children as well as her grandchildren, but without any support or access to mental health services, life in the community has been a struggle for her.
Strangely — and tragically — prison represented a respite for Merri. With eyes glistening with tears, she told me: “[Prison] is very stressful. But I’m finding it a break from a lot of stress outside.”
Today, on International Women’s Day, the Australian government should commit to making it a priority to meet the needs of women with disabilities who are at risk of violence and abuse.
In 2015, a Senate inquiry into the abuse people with disabilities face in institutional and residential settings revealed the extensive and diverse forms of abuse they face both in institutions and the community. The inquiry recommended that the government set up a Royal Commission to conduct a more comprehensive investigation into the neglect, violence, and abuse faced by people with disabilities across Australia.
While the framework is an important step forward, it would only reach people who are enrolled under the NDIS. Its complaints mechanism would not provide a comprehensive look at the diversity and scale of the violence people with disabilities experience, let alone at the ways in which various intersecting forms of discrimination affect people with disabilities.
The creation of a Royal Commission, on the other hand, could give voice to survivors of violence inside and outside the NDIS. It could direct a commission’s resources at a thorough investigation into the violence people with disabilities face in institutional and residential settings, as well as in the community.
The government urgently needs to hear directly from women like Merri about the challenges they face, and how the government can do better at helping them. Whether or not there is a Royal Commission, the government should consult women with disabilities, including Indigenous women, and their representative organizations to learn how to strengthen support services.
Government services that are gender and culturally appropriate, and accessible to women across the country, can curtail abuse and allow women with disabilities to live safe, independent lives in the community.
Kriti Sharma is a disability rights researcher for Human Rights Watch
How you can support #JustJustice
• Download, read and share the 2nd edition – HERE.
• Buy a hard copy from Gleebooks in Sydney (ask them to order more copies if they run out of stock).
• Send copies of the book to politicians, policy makers and other opinion leaders.
• Encourage journals and other relevant publications to review #JustJustice.
• Encourage your local library to order a copy, whether the free e-version or a hard copy from Gleebooks.
” The many years of community-generated work in suicide prevention is something that Indigenous Australia, as a collective, should take great pride in.
However, we have to acknowledge also that this alone has not been enough to stop Indigenous suicide rates overall getting higher recently, and that some communities remain at particularly high risk.
ATSISPEP’s first challenge was to identify ‘what works:’ the success factors evident from the suicide prevention work already undertaken in our communities. The second challenge was to support the dissemination of ‘what works’ across all communities: to share knowledge, and ensure that all can benefit from this collective wisdom and experience.”
Professor Pat Dudgeon and Professor Tom Calma AO Website
Photo above : Page 15 NACCHO Aboriginal Health Newspaper to be published 16 November
The Aboriginal and Torres Strait Islander Suicide Prevention Evaluation Project (ATSISPEP) is a unique Indigenous-led research project to identify ‘what works’ to prevent suicide in our communities.
At launch at Parliament House with politicians from all parties and special guests the family of Norma from Leonora who lost a son not long ago and Lena from Fitzroy Crossings who lost a daughter.
Our rates of suicide today are twice as high as other Australians and probably growing. Like the tip of an iceberg, high rates of suicide in a community can be a sign of deeper and complex community-wide problems, involving families and people caught in cycles of despair and a sense of hopelessness. Yet not all our communities, even those facing similar challenges, experience the same rates of suicide.
ATSISPEP was developed with the recognition that for many years Indigenous Elders, community leaders and healers in some of our worst-affected communities have been working tirelessly to prevent suicide.
Often volunteering, and with little or no financial support, they have generated community-specific and culturally-based ways of bringing people back from the edge of suicide and also supporting families who are bereaved by loss.
In some cases, they have worked with entire communities to address the underlying community-level issues that can contribute to a suicide, for example, unemployment, violence, and alcohol and drug use. In others, they have connected young people to their Indigenous identity and culture and the sense of worth this can bring.
The many years of community-generated work in suicide prevention is something that Indigenous Australia, as a collective, should take great pride in.
However, we have to acknowledge also that this alone has not been enough to stop Indigenous suicide rates overall getting higher recently, and that some communities remain at particularly high risk.
ATSISPEP’s first challenge was to identify ‘what works:’ the success factors evident from the suicide prevention work already undertaken in our communities. The second challenge was to support the dissemination of ‘what works’ across all communities: to share knowledge, and ensure that all can benefit from this collective wisdom and experience.
The report includes an analysis of Indigenous suicide prevention program evaluations and previous research and consultations on Indigenous suicide prevention. It includes the input of ATSISPEP-held regional community roundtables, and roundtables on specific topics (for example, on Indigenous young people and suicide prevention, justice issues, and Indigenous LGBTQI and suicide prevention).
ATSISPEP also held a national conference in Alice Springs this May. It was an opportunity to test our work and gather even more information from the 370 attendees, most of whom were Indigenous.
A selection of some of the success factors identified in the report includes:
Community-specific programs to address the community-level contributing factors that can lead to suicide.
Community development and ownership of programs.
Access to culturally competent counsellors and mental health support for people at immediate risk of suicide.
The involvement of Elders in programs.
Cultural frameworks for programs, and cultural elements in them: for example, culturally-informed healing practices and connecting young people to country.
Alcohol and drug use-reduction as a part of an overall response.
Gatekeeper training, whereby community members are trained to identify people at risk of suicide and connect them to help.
For young people, peer to peer mentoring, and education and leadership on suicide prevention.
24-hour, seven-day a week availability of support.
With ATSISPEP complete, the implementation of the 2013 National Aboriginal and Torres Strait Islander Suicide Prevention Strategy (with almost $18 million pledged to it) through the Primary Health Networks, and the establishment of at least two Indigenous suicide prevention trial sites (that were recently announced by the Australian Government) can proceed on an evidence-based footing. ATSISPEP has also generated tools for both Indigenous communities and Primary Health Networks to use to develop and strengthen programs.
Our NACCHO CEO Pat Turner as a contributor to the report attended the launch pictured here with Senator Patrick Dodson and co-author Prof. Pat Dudgeon
The hope of ATSISPEP is that its report will help bring about a new era in Indigenous suicide prevention in which many lives will be saved. It is now incumbent on Australian governments to ensure that our communities receive the support they need to help make this happen.
ATSISPEP was funded by the Commonwealth Department of Health.
If you are looking for help please call one of the following national helplines:
Lifeline Counselling Service: 13 11 14; Suicide Call Back Service: 1300 659 467 (cost of a local call)