Racism causes stress – stress is one of the most powerful contributors to illness and poor health.
Racism causes people to self-medicate with things like drugs and alcohol
Racism makes me sick. It makes Sam sick.
It makes everyone who is the target of it sick. It is one of the key reasons why the health gap in Australia is so wide.
Racism a driver of Aboriginal ill health See previous ARTICLE
EXCLUSIVE COLUMN: SOL Bellear, the long-serving chairperson of the Aboriginal Medical Service, Redfern, takes a swipe at Brisbane star Sam Thaiday.
PICTURE Above AIATSIS
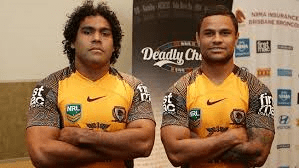
LATE this week, the Brisbane Broncos unveiled their special Indigenous jersey, a strip designed to honour the contribution of past and current players, and in particular to highlight efforts to ‘Close the Gap’ in Indigenous health.
It’s a great initiative, and not before time.
But for me at least, the event was soured by the comments of Broncos’ star, Sam Thaiday.(picture above left)
I have enormous admiration and respect for Sam. He’s been a great contributor to rugby league and a role model to kids all over Australia. But Sam’s views on racism – that the best way to confront it is to “push it aside” – don’t sit well with me
At the jersey launch, Sam told media: “We’re out there to win at all costs and sometimes things get said in the heat of the moment that I think aren’t said as a hurtful thing.
“It is a tough thing to hear but you can’t really react to those things these days. I think the best way to deal with it is to try and push it aside as much as possible.”
Sorry Sam. That’s no solution at all.
There is never any excuse for racism, no matter how it is said, no matter how it meant. It is unacceptable in any form.
There are countless reasons why, but the most compelling is precisely one of the reasons why the Broncos launched the jersey in the first place – to highlight the gap in Indigenous health.
Racism makes me sick. It makes Sam sick. It makes everyone who is the target of it sick. It is one of the key reasons why the health gap in Australia is so wide.
For example, countless studies have shown significantly higher rates of smoking among the poor (it’s 50 percent among us blackfellas). And whatever your views about modern Indigenous politics, I challenge anyone to make a case that the poverty suffered by Indigenous Australians today is not a direct result of the racism of our past.
The racism of our present may be less overt, but it still hurts
Racism causes stress – stress is one of the most powerful contributors to illness and poor health.
Racism causes people to self-medicate with things like drugs and alcohol.
The simple reality is that racism affects everyone in this country, and no problem ever went away by “pushing it aside”, as Sam suggests.
As a role model, Sam and other Indigenous players of the NRL have a responsibility to stand up to it whenever they see it.
Related articles
- NACCHO NRL Close the Gap round: NRL players Indigenous DADS hopes and dreams for healthy kids (nacchocommunique.com)
- NACCHO congratulates the NRL for support of the OXFAM Close the Gap round (nacchocommunique.com)
- NACCHO NASTIHP health plan news: Racism a driver of Aboriginal ill health (nacchocommunique.com)
- Racism not intentional in NRL: Thaiday (news.theage.com.au)
- NACCHO NATSIHP news: $12 billion Aboriginal health plan to be launched today (nacchocommunique.com)
- Thaiday says NRL racism not intentional (bigpondnews.com)
- NACCHO OCHRE DAY:The new generation of Aboriginal males is making generational changes (nacchocommunique.com)