This weeks #ACCHO #Jobalerts
Please note : Before completing a job application please check with the ACCHO that the job is still open
This weeks #ACCHO #Jobalerts
Please note : Before completing a job application please check with the ACCHO that the job is still open
Job of the Week- Permanent General Practitioner – Gladstone

Description:
Gladstone on the Central Queensland Coast.
Gladstone sits at the start of the Great Barrier Reef, and our beautiful Harbour is surrounded by a multitude of easily accessible islands, for camping, fishing or resort style. Gladstone incorporates the seaside towns of Boyne Island and Tannum Sands, as well as Calliope. Gladstone is easy driving distance to Rockhampton, one hour to the north, or southeast to historic Bundaberg, Agnes Waters and the town of 1770 is a two hour drive away.
The position is within a group Practice for a full time General Practitioner at the local Aboriginal and Islander Community Controlled Health Service. The practice is in the central business district of the town, in a new, purpose built facility. It is a bulk billing practice with online claiming. The role is fully supported by a an experienced, multidisciplinary health team consisting of a Clinical Practice Manager, Registered Nurses, Aboriginal Health Workers and Medical Receptionists.
The Practice is further supported by visiting allied health professionals – podiatry, exercise physiology, diabetic educator and visiting specialists in mental health, endocrinology, paediatrics and cardiology. The health service provides comprehensive primary health care services, with targeted programs for Aboriginal and Torres Strait Islander health, preventative health, chronic disease management, maternal and child health, tobacco cessation, aged care and healthy lifestyles. There is a desire to open for a half day Saturday.
There are no scheduled out of hour’s requirements. Attendance at community events may be required on an occasional weekend. This position is 40 hours per week, Monday to Friday. No on call requirements.
Attractive salaried remuneration package with salary sacrifice, four weeks annual leave and one weeks professional development paid leave per year. Accommodation paid for 6 – 12 months in a fully furnished house/apartment – negotiable on longevity of placement.
There is a large range of both public and private schools for primary and secondary schooling, a campus of Central Qld University/CQ Tafe offering a wide variety of higher education as well as a dedicated Technical College at Gladstone State High School.
The area offers plenty of sporting and recreational activities and opportunities, and has a dedicated entertainment and restaurant precinct. With parks, playgrounds, sporting venues, islands, beaches and beautiful weather, this town offers you everything.
Requirements of the position:
- Current and unconditional registration with AHPRA
- Fellowship with RACGP or ACRRM
- Ability to pass a federal police check
If you are an enthusiastic General Practitioner who would like to make a real difference in people’s lives, would like to be part of an experienced, supportive team of health care providers, this Medical Health Service is for you.
Job ID 1777
Following successful placement eligible candidates may be entitled to receive support and financial assistance through Health Workforce Queensland’s comprehensive workforce attraction and retention incentives.
Contact: 07 3105 7800
QAIHC Sexual Health Coordinator

QAIHC is a non-partisan peak organisation representing 28 Aboriginal and Islander Community Controlled Health Organisations (AICCHOs) across Queensland at both state and national level. Our members deliver comprehensive and culturally appropriate, world class primary health care services to their communities.
Role Overview
- Based in the QAIHC Cairns office
- Salary $82,500 + superannuation + attractive health promotion charity salary packaging
- Temporary role contracted till 31st December 2019
The Sexual Health Coordinator Role is a project-based role that is being funded by Queensland Health under their Making Tracks Indigenous Investment Strategy. As part of this project, the Sexual Health Coordinator would assist with the coordination of sexual health service delivery across AICCHO’s within North Queensland and provide support and resources in developing and delivering their Sexual Health programs at the local level.
The Sexual Health Coordinator will be a central role in a project designed to:
- Implement a coordinated response to ensure the reduction of STIs among Aboriginal and Torres Strait Islander people in North Queensland.
- Improve the knowledge and awareness of STIs and protective behaviours among Aboriginal and Torres Strait Islander people in North Queensland particularly those under 30 years of age, through the delivery of evidence based, culturally appropriate sexual health promotion.
- Improve access to and delivery of culturally secure STI services, including best practice STI testing and management.
- Improve the knowledge and skills of the workforce to provide culturally secure services and appropriate models of care for delivery of STI services to Aboriginal and Torres Strait Islander people.
- Establish data collection and surveillance systems to enable the effective review of progress and improvement towards achieving the goals of the action plan.
Pre-requisite skills & experience
-
- High level knowledge of sexual health issues, treatment and prevention
- Qualifications in health promotion, public health, social science (with a health promotion major), health education or related field or relevant experience.
- Ability to build relationships and engage with a broad range of stakeholders.
- High level communication, collaboration and interpersonal skills.
- Understanding of the Aboriginal and Torres Strait Islander Community Controlled Health Organisations and the issues facing them.
- Ability to work with Aboriginal and Torres Strait Islander communities and their leaders, respecting traditional culture, values and ways of doing business.
- A current drivers licence
- Aboriginal and Torres Strait Islander people are strongly encouraged to apply for this position
To apply, obtain an application pack or any query, please email – applications@qaihc.com.au.
Please apply only via this method.
Applications are required by midnight on Sunday 29th July 2018
Clinical Trainer – Aboriginal Health Primary Healthcare Practice
VICTORIAN ABORIGINAL COMMUNITY CONTROLLED HEALTH ORGANISATION

VACCHO is Victoria’s peak representative Aboriginal health body and champions community control and health equality for Aboriginal communities. We are a centre of expertise, policy advice, training, innovation and leadership in Aboriginal health. VACCHO advocates for the health equality and optimum health of all Aboriginal people in Victoria.
Our Education and Training Unit (ETU) is a Registered Training Organisation (RTO) and VACCHO strives to operate as a dynamic and responsive provider of vocational education and training to the Aboriginal Community Controlled Health sector.
We are looking for someone to deliver training and assess competency against the Aboriginal Health Care qualifications from AQF level II to Diploma. This is a fantastic opportunity for someone passionate about health to educate the next generations of practitioners and assist in improving community health, well-being and contributing to promoting healthier lifestyles.
Aboriginal and/or Torres Strait Islander people are strongly encouraged to apply, but also suitable for someone with relevant experience working in community.
You will need:
- Certificate IV in Training and Assessment (although we can assist in obtaining this for the right candidate)
- Qualifications in health or primary health care related fields to a minimum of ACF level V
- Clinical experience or practice in Aboriginal health or non-Aboriginal health, acute, primary or community health settings
- Current registration with Australian Health Practitioner Regulation Agency (AHPRA).
If this sounds like the job you are looking for then you can download the Position Description and application form from our website http://www.vaccho.org.au/jobs.
To apply please email a copy of your resume and application form to employment@vaccho.org.au
For queries about the position please contact Helen Grose on 9411 9411. Applications close on Tuesday 24 July.
DYHSAC is currently seeking suitably experienced Governance Support Officer

About the Organisation
The name Derbarl Yerrigan is the Wadjuk Noongar name for the Swan River. Derbarl Yerrigan Health Service Aboriginal Corporation (DYHSAC) has a proud history of providing Aboriginal health services within the Perth metropolitan area and in 1974 was the first Aboriginal Community Controlled Health Service to be established in Australia. DYHSAC has now grown to have four successful, busy clinics across the Perth metro area, delivering comprehensive healthcare and specialised programs along with an accommodation centre for clients requiring medical treatment away from home or Country. Our mission is to provide high quality, holistic and culturally secure health services for Aboriginal and Torres Strait Islander people and communities in the Perth metropolitan region.
About the Opportunity
DYHSAC is currently seeking suitably experienced Governance Support Officer to join our team on a 12 months Fixed term Full time contract . Reporting to the Chief Executive Officer, the Governance Support Officer is responsible for providing administrative support to the CEO, Board Secretariat and Executive Officer as a crucial part of the Office of the CEO.
Please note: Aboriginal and/or Torres Strait Islander people are highly encouraged to apply for this position.
Primary responsibilities include but are not limited to:
- Provide administrative support to the Board Secretariat in the conduct of DYHSAC Board and Sub-committee meetings and assist with the implementation and follow up of Board and Sub-Committee resolutions, recommendations and actions.
- Accurately maintain governance and Board information including Board decision and information papers, registers, policies, procedures and associated documents including those required under the Corporations (Aboriginal and Torres Strait Islander) Act 2006 (CATSI Act).
- Contribute to the successful operation of the Office of the CEO through the provision of high quality support services.
- Attend and take minutes of other internal meetings.
About the Successful Person
You will have:
- Demonstrated understanding of the unique issues affecting and impacting on the health and wellbeing of Aboriginal people.
- Highly developed communication skills, including an ability to communicate effectively and sensitively with Aboriginal people.
- Demonstrated ability to manage and maintain strict confidentiality at all times.
- High level verbal and written communication skills with strong attention to detail.
- Demonstrated ability to use computers and related software packages, specifically MS Word, Outlook, Excel and Power Point.
- Ability to take minutes in a formal meeting environment.
- Ability to work with minimum supervision to meet deadlines and daily work commitments.
- Ability to undertake basic research and prepare draft correspondence, reports and written documentation.
- It is an essential requirement for this position to undertake a National Police Check.
About the Benefits
- Competitive salary + superannuation + salary sacrificing.
All applications are to be submitted via the below link only. Email and hard copy applications will not be accepted.
Closing date: Friday 20 July 2018
ONLY short-listed applicants will be contacted. Interviews may commence prior to the advertisement closing.
Please note that the Derbarl Yerrigan Health Service Aboriginal Corporation is an equal opportunity institution, providing educational and employment opportunities without regard to race, colour, gender, age, or disability.
Community Support Officer MAMU HEALTH SERVICE LIMITED

Mamu Health Service Limited is an Aboriginal community controlled health service providing comprehensive primary health care services to the Aboriginal and Torres Strait Islander communities in Innisfail and surrounding districts. We are recruiting the following position:-
Community Support Services Manager – Providing leadership within the Community Support Services programs and working collaboratively with Senior Management Team. Minimum qualification – Diploma level or higher and previous Management in Counselling/Drug and Alcohol
All applicants must be willing to undertake an AFP Criminal History Check, and a Blue Card with Commission for Children and Young People and Child Guardian.
To apply for this vacancy, a full application package can be obtained from our website on www.mamuhsl.org.au, or please don’t hesitate to contact Julie Browne on 07 4061 9988 or jbrowne@mamuhsl.org.au to register your interest.
Please submit your resume and written responses addressing the Knowledge, Skills and Personal Attributes outlined in the Position Description to:
The Chief Executive Officer
Mamu Health Service Limited
PO Box 1537
INNISFAIL Q 4860
Applications close at 5.00 pm on Friday 20th July 2018
It is a genuine occupational requirement that that the position be filled by an Aboriginal or Torres Strait Islander person as permitted by Section 25, 105 & 106 Queensland Anti-Discrimination (1991) Act.
Deputy CEO Danila Dilba ACCHO Darwin Closing 15 June

About the Organisation
Danila Dilba Health Service is an Aboriginal community-controlled organisation providing culturally-appropriate, comprehensive primary health care and community services to Biluru (Aboriginal and Torres Strait Islander) people in the Yilli Rreung (greater Darwin) region of the Northern Territory.
The mission of DDHS is to improve the physical, mental, spiritual, cultural and social wellbeing of its clients through innovative comprehensive primary health care programs that are based on the principles of equity, access, empowerment, community self-determination and inter-sectoral collaboration.
About the Opportunity
Danila Dilba now has an exciting leadership opportunity for a full-time Deputy CEO to join their team in Darwin.
Working closely with the CEO, this role will see you responsible for providing strong internal leadership and day to day management to Corporate Services, enabling the organisation to achieve its strategic and operational goals. You will also ensure the effective communication of the organisation’s vision and strategies.
Some key duties will include (but will not be limited to):
- Leading an advocacy agenda to influence decision makers on policy issues related to Aboriginal health and wellbeing;
- Assisting the Board and CEO in implementing the strategic and business plans including engagement of stakeholders and delivering organisational objectives;
- Providing line management to the HR, Finance, Audit and Compliance, Facilities Management, and ICT functions of the business;
- Leading growth and sustainability through development and implementation of a Business Development Strategy targeting emerging opportunities, innovations and potential income streams;
- Developing and strengthening strategic stakeholder relationships and partnerships; and
- Taking responsibility for service quality and continuous improvement.
This is an identified Aboriginal position; exemption is claimed under Section 8 (1) of the Racial Discrimination Act 1975.
About the Benefits
This is a fantastic opportunity to take on a new leadership challenge within a fast-paced and expanding organisation!
Danila Dilba Health Service offers a stable, safe and supportive work environment with plenty of challenges and variety as you interact with people from a wide range of cultural and social backgrounds.
Danila Dilba Health Service is an organisation that truly values its team, and is committed to improving employee knowledge, skills and experience. Staff development programs are both encouraged and provided by the organisation.
You will receive a competitive remuneration (negotiable with experience and qualifications)PLUS super, phone, laptop, salary sacrificing options and a range of benefits including:
- 6 weeks annual leave per year (with the opportunity to cash-out up to two weeks annual leave in any financial year);
- Relocation assistance (negotiable) when relocating to Darwin;
- Fully maintained vehicle for private use;
- Up to 2 weeks paid study leave per annum;
- Professional development and training provided; and
- Entertainment benefits (up to $2,550).
Most importantly, you’ll be joining a team of passionate and dedicated individuals who contribute to the positive impact made on the local community. Here you will be able to voice your thoughts and opinions, as the organisation embraces opportunity and encourages its people to initiate action and follow through on the outcome.
How to Apply
Take on a new challenge in your executive career, with a progressive Aboriginal community-controlled organisation – Apply Now!

Mallee District Aboriginal Services Victoria
MDAS has opportunities for highly-motivated and organised individuals looking to work as part of a professional team committed to improving Aboriginal health and wellbeing.
Aboriginal and Torres Strait Islander People are strongly encouraged to apply for all positions.
MDAS is committed to protecting children and young people from harm. We require all applicants who are to work with children and young people to undergo an extensive screening process prior to appointment, a process that includes, but is not limited to, comprehensive reference checks, an identity check, a ‘working with children’ check and/or a ‘national criminal history record’ check.
MDAS is proud to be a LGBTI-friendly workplace.
This page is updated weekly.
This page is updated weekly.

How to submit a Indigenous Health #jobalert ?
NACCHO Affiliate , Member , Government Department or stakeholders
If you have a job vacancy in Indigenous Health
Email to Colin Cowell NACCHO Media
Tuesday by 4.30 pm for publication each Wednesday
There are 3 JOBS AT Apunipima Cairns and Cape York



There are 8 JOBS AT IUIH Brisbane and throughout Queensland
+ Nurse Home Visitor (2 x Ongoing, Full Time Positions based on Northside and Southside) + Family Partnership Worker (2 x Ongoing, Full Time Positions based on Northside and Southside) + Medical Quality Coordinator (Ongoing, Full Time Position based in Strathpine) + Deadly Choices Program Officer (Several Ongoing, Full Time positions across SEQ) + Deadly Choices Program Officer – MATSICHS (Several Ongoing, Full Time
There are 14 jobs at ATSICHS Brisbane

As part of our commitment to providing the Aboriginal and Torres Strait Islander community of Brisbane with a comprehensive range of primary health care, youth, child safety, mental health, dental and aged care services, we employ approximately 150 people across our locations at Woolloongabba, Woodridge, Northgate, Acacia Ridge, Browns Plains, Eagleby and East Brisbane.
The roles at ATSICHS are diverse and include, but are not limited to the following:
- Aboriginal Health Workers
- Registered Nurses
- Transport Drivers
- Medical Receptionists
- Administrative and Management roles
- Medical professionals
- Dentists and Dental Assistants
- Allied Health Staff
- Support Workers
NT Jobs of the week 40 positions in the NT Alice Spring ,Darwin East Arnhem Land and Katherine
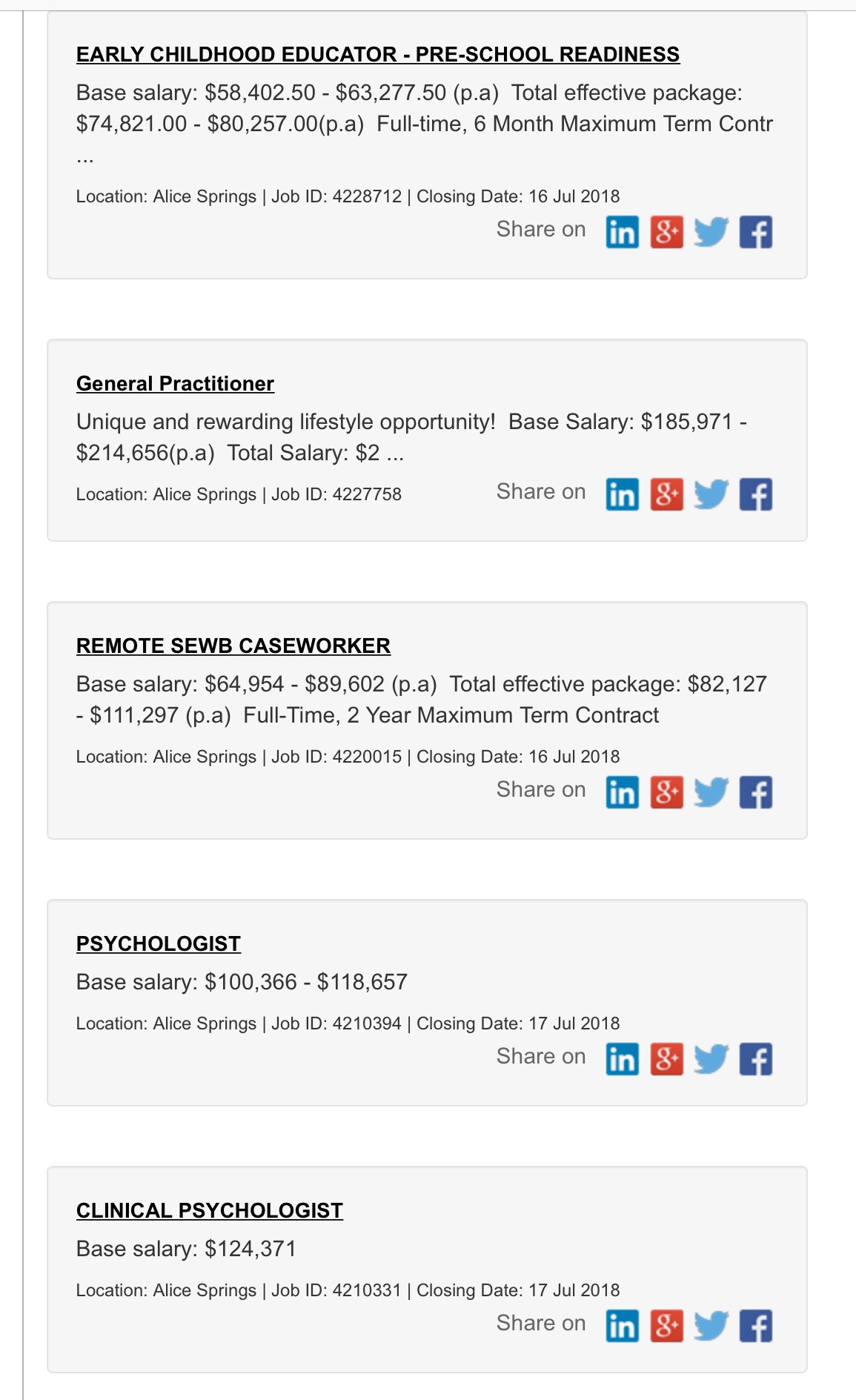
There are 13 JOBS at Congress Alice Springs including




There are 17 JOBS at Miwatj Health Arnhem Land


There are 2 JOBS at Wurli Katherine