
55 leaders met today 9th of June 2016, in Redfern where in 1992 Prime Minister Paul Keating spoke truth about this nation – that the disadvantage faced by First Peoples affects and is the responsibility of all Australians.
Photo above NACCHO CEO Pat Turner addressing the national media
An urgent call for a more just approach to Aboriginal and Torres Strait Islander Affairs
“Social justice is what faces you in the morning. It is awakening in a house with adequate water supply, cooking facilities and sanitation. It is the ability to nourish your children and send them to school where their education not only equips them for employment but reinforces their knowledge and understanding of their cultural inheritance. It is the prospect of genuine employment and good health: a life of choices and opportunity, free from discrimination.”
Mick Dodson, Annual Report of the Aboriginal and Torres Strait Islander Social Justice Commissioner, 1993.
The Redfern Statement
Download the 18 Page document here
Redfern Statement June 2016 Elections 18 Pages

A call for urgent Government action
In the past 25 years – a generation in fact – we have had the Royal Commission into Aboriginal Deaths in Custody, the Bringing them home Report and Reconciliation: Australia’s Challenge: the final report of the Council for Aboriginal Reconciliation. These reports, and numerous other Coroner and Social Justice Reports, have made over 400 recommendations, most of which have either been partially implemented for short term periods or ignored altogether.
In the last 25 years we have seen eight Federal election cycles come and go, with seven Prime Ministers, seven Ministers for Indigenous Affairs, countless policies, policy changes, funding promises and funding cuts – all for the most marginalised people in Australia.
For the last quarter century, then, we’ve seen seminal reports which have repeatedly emphasised that our people need to have a genuine say in our own lives and decisions that affect our peoples and communities. This, known as self-determination, is the key to closing the gap in outcomes for the First Peoples of these lands and waters.
All of these reports call for better resourcing of Aboriginal and Torres Strait Islander organisations and services for Aboriginal and Torres Strait Islander communities.
All of these reports call for real reconciliation based on facing the truths of the past and creating a just and mature relationship between the non-Indigenous Australian community and the First Peoples.
The next Federal Government will take on the same responsibility to right this nation’s past injustices as the last eight Federal Governments have had. The next Government of Australia will take power with our First Peoples facing the same struggles as they were in 1992. But this next Federal Government also has an unprecedented nation-building opportunity to meaningfully address Aboriginal and Torres Strait Islander disadvantage. They have the mandate to act. We therefore call on the next Federal Government to:
- Commit to resource Aboriginal and Torres Strait Islander led-solutions, by:
- Restoring, over the forward estimates, the $534 million cut from the Indigenous Affairs portfolio in the 2014 Budget to invest in priority areas outlined in this statement; and
- Reforming the Indigenous Advancement Strategy and other Federal funding programs with greater emphasis on service/need mapping (through better engagement) and local Aboriginal and Torres Strait Islander organisations as preferred providers.
- Commit to better engagement with Aboriginal and Torres Strait Islander peoples through their representative national peaks, by:
- Funding the National Congress of Australia’s First Peoples (Congress) and all relevant Aboriginal and Torres Strait Islander peak organisations and forums; and
- Convening regular high level ministerial and departmental meetings and forums with the Congress and the relevant peak organisations and forums.
- Recommit to Closing the Gap in this generation, by and in partnership with COAG and Aboriginal and Torres Strait Islander people:
- Setting targets and developing evidence-based, prevention and early intervention oriented national strategies which will drive activity and outcomes addressing:
- family violence (with a focus on women and children);
- incarceration and access to justice;
- child safety and wellbeing, and the over-representation of Aboriginal and Torres Strait Islander children in out-of-home care; and
- increasing Aboriginal and Torres Strait Islander access to disability services;
- Secure national funding agreements between the Commonwealth and States and Territories (like the former National Partnership Agreements), which emphasise accountability to Aboriginal and Torres Strait Islander peoples and drive the implementation of national strategies.
- Commit to working with Aboriginal and Torres Strait Islander leaders to establish a Department of Aboriginal and Torres Strait Islander Affairs in the future, that:
- Is managed and run by senior Aboriginal and Torres Strait Islander public servants;
- Brings together the policy and service delivery components of Aboriginal and Torres Strait Islander affairs and ensures a central department of expertise.
- Strengthens the engagement for governments and the broader public service with Aboriginal and Torres Strait Islander people in the management of their own services.
- Commit to addressing the unfinished business of reconciliation, by:
- Addressing and implementing the recommendations of the Council for Aboriginal Reconciliation, which includes an agreement making framework (treaty) and constitutional reform in consultation with Aboriginal and Torres Strait Islander peoples and communities.
The health and wellbeing of Aboriginal and Torres Strait Islander peoples cannot be considered at the margins.
It is time that Aboriginal and Torres Strait Islander voices are heard and respected, and that the following plans for action in relation to meaningful engagement, health, justice, preventing violence, early childhood and disability, are acted upon as a matter of national priority and urgency.
National Representation for Aboriginal and Torres Strait Islander Peoples
It is critical that Australia’s First Peoples are properly represented at the national level to ensure meaningful engagement with Government, industry and the non-government sectors to advance the priorities of our people.
Since 2010, the National Congress of Australia’s First Peoples (Congress) has gone some way to fill the gap in national representation since the demise of the Aboriginal and Torres Strait Islander Commission in 2005.
However, there remain too many gaps in adequate national level representation for Aboriginal and Torres Strait Islander people – particularly for employment and education. Without Congress or equivalent national bodies where Aboriginal and Torres Strait Islander leaders are supported to engage with Government it will be difficult for the next Federal Parliament to meet the multi-partisan priority and commitment to work ‘with’ Aboriginal and Torres Strait Islander people.
We call on the next Federal Government to commit to:
- Restoration of funding to the National Congress of Australia’s First Peoples
The National Congress of Australia’s First Peoples (Congress) was established in 2010 to be the representative voice of Aboriginal and Torres Strait Islander peoples and to advocate for positive change. The decision to defund Congress, just as it is beginning to emerge as a unifying element among Aboriginal and Torres Strait Islander groups, is a mistake.
Without support, Congress’ ability to do its job of representing Aboriginal and Torres Strait Islander interests is severely compromised. Congress must be supported to provide a mechanism to engage with our people, develop policy, and advocate to Government.
Congress should be supported to reach sustainability and independence as soon as possible.
- A national Aboriginal and Torres Strait Islander representative body for Education
Although there are many good quality Aboriginal and Torres Strait Islander organisations, and strong leaders, working at the State and local level in the education sector, there is currently no national body to promote and engage in education policy for Australia’s First Peoples.
The education sector is fragmented across early childhood, primary and secondary education, vocational education and training, and higher education, with each of state and territory having public, catholic and private school systems. In the absence of a single national education voice for Aboriginal and Torres Strait Islander people, Congress has been active in coordinating and promoting unity across these sectors. Congress has consulted widely with its members, educators and organisations, many of which have a long history of working in this area.
We call on the next Federal Government to establish a national body that can call for policies support Aboriginal and Torres Strait Islander students and communities across all of these educational systems.
- A national Aboriginal and Torres Strait Islander representative body for Employment
The highly disadvantaged employment and income status of Aboriginal and Torres Strait Islander peoples is well documented. While we appreciate attempts at advancing opportunities for Aboriginal and Torres Strait Islander peoples, the many issues around employment require a unified and expert voice.
Beyond skills training, mentoring and targeted employment services to enhance the job readiness of
Aboriginal and Torres Strait Islander peoples, concerted effort needs to be directed to creating jobs that are suitable and meaningful for our people. This is of particular concern in remote areas, where mainstream commercial and labour market opportunities are limited. In urban and rural areas, Aboriginal and Torres Strait Islander people are faced with issues of racism and discrimination in the workplace.
The next Federal Government should establish and fund a national representative body of Aboriginal and Torres Strait Islander leaders to drive employment and economic solutions for our people, in order to:
- Work with our communities to develop their own strategies for economic development, and promote community participation and management;
- Promote strategies to create Aboriginal and Torres Strait Islander-friendly workplaces; and
- Work with Government to design welfare policy that encourages, rather than coerces, Aboriginal and Torres Strait Islander peoples into employment.
-
- A national Aboriginal and Torres Strait Islander representative body for Housing
Federal and State Government policies concerning Aboriginal and Torres Strait Islander housing is currently disjointed, wasteful and failing. For example, Aboriginal and Torres Strait Islander people in urban and regional markets face many barriers in accessing and securing safe and affordable housing, including discrimination and poverty.
The next Federal Parliament should support the development of a national representative body of Aboriginal and Torres Strait Islander leaders who can focus on housing security for Aboriginal and Torres Strait Islander peoples, and:
- Advocate for the ongoing support for remote communities to prevent community closures;
- Work with communities to develop a national Aboriginal and Torres Strait Islander housing strategy, with the aim of improving the housing outcomes for our people across all forms of housing tenure; and
- Provide culturally appropriate rental, mortgage and financial literacy advice.
First Peoples Health Priorities
Closing the Gap in health equality between Aboriginal and Torres Strait Islander people and non-Indigenous Australians is an agreed national priority. The recognised necessity and urgency to close the gap must be backed by meaningful action.
All parties contesting the 2016 Federal Election must place Aboriginal and Torres Strait Islander affairs at the heart of their election platforms, recognising the health equality as our national priority.
Despite the regular upheaval of major policy changes, significant budget cuts and changes to Government in the short election cycles at all levels, we have still managed to see some encouraging improvements in Aboriginal and Torres Strait Islander health outcomes. But much remains to be achieved and as we move into the next phase of Closing the Gap, enhanced program and funding support will be required.
We appeal to all political parties to recommit to Closing the Gap and to concentrate efforts in the priority areas in order to meet our goal of achieving health equality in this generation.
We call on the next Federal Government to commit to:
- Restoration of funding
The 2014 Federal Budget was a disaster for Aboriginal and Torres Strait Islander people. This is not an area where austerity measures will help alleviate the disparity in health outcomes for Australia’s First Peoples.
The current funding for Aboriginal health services is inequitable. Funding must be related to population or health need, indexed for growth in service demand or inflation, and needs to be put on a rational, equitable basis to support the Implementation Plan for the National Aboriginal and Torres Strait Islander Health Plan (2013–2023).
- Fund the Implementation Plan for the National Aboriginal and Torres Strait Islander Health Plan (2013–2023)
Future Budgets must adequately resource the Implementation Plan’s application and operation. As a multi-partisan supported program, the Implementation Plan is essential for driving progress towards the provision of the best possible outcomes from investment in health and related services.
- Make Aboriginal Community Controlled Services (ACCHS) the preferred providers
ACCHS should be considered the ‘preferred providers’ for health services for Aboriginal and Torres Strait Islander people. Where there is no existing ACCHS in place, capacity should be built within existing ACCHS to extend their services to the identified areas of need. This could include training and capacity development of existing services to consider the Institute of Urban Indigenous Health strategy to self-fund new services. Where it is appropriate for mainstream providers to deliver a service, they should be looking to partner with ACCHS to better reach the communities in need.
- Create guidelines for Primary Health Networks
The next Federal Government should ensure that the Primary Health Networks (PHNs) engage with ACCHS and Indigenous health experts to ensure the best primary health care is delivered in a culturally safe manner. There should be mandated formal agreements between PHNs and ACCHS to ensure Aboriginal and Torres Strait Islander leadership.
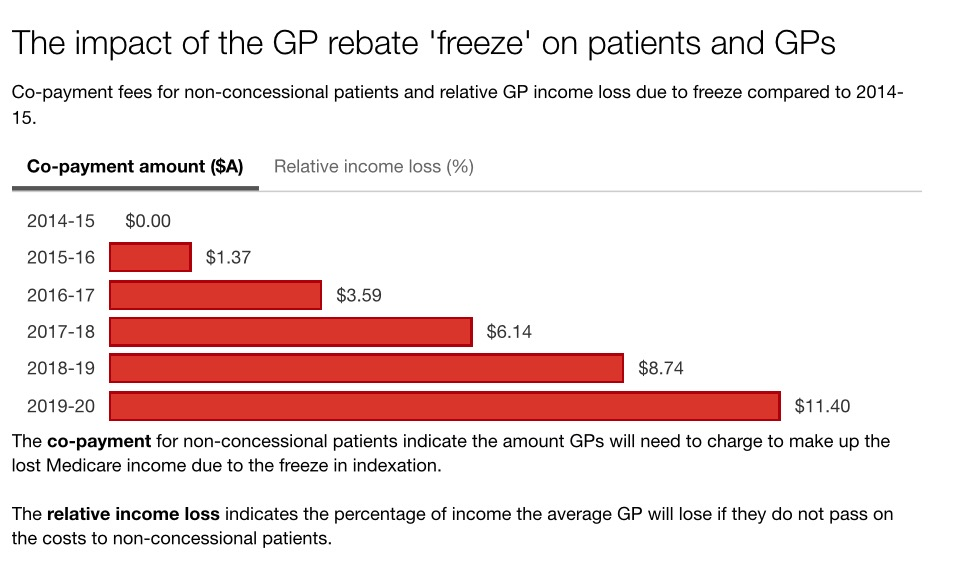
- Resume indexation of the Medicare rebate, to relieve profound pressure on ACCHS
The pausing of the Medicare rebate has adversely and disproportionately affected Aboriginal and Torres Strait Islander people and their ability to afford and access the required medical care. The incoming Federal Government should immediately resume indexation of Medicare to relieve the profound pressure on ACCHS.
- Reform of the Indigenous Advancement Strategy
The issues with the Indigenous Advancement Strategy (IAS) are well known. The recent Senate Finance and Public Administration Committee Report into the tendering processes highlighted significant problems with the IAS programme from application and tendering to grant selection and rollout.
The next Federal Government must fix the IAS as an immediate priority and restore the funding that has been stripped from key services through the flawed tendering process.
- Fund an Implementation Plan for the National Aboriginal and Torres Strait Islander Suicide Prevention Strategy
The National Aboriginal and Torres Strait Islander Suicide Prevention Strategy encompasses Aboriginal and Torres Strait Islander peoples’ holistic view of mental health, as well as physical, cultural and spiritual health, and has an early intervention focus that works to build strong communities through more community-focused and integrated approaches to suicide prevention.
The Strategy requires a considered Implementation Plan with Government support to genuinely engage with Aboriginal and Torres Strait Islander communities, their organisations and representative bodies to develop local, culturally appropriate strategies to identify and respond to those most at risk within our communities.
- Develop a long-term National Aboriginal and Torres Strait Islander Social Determinants of Health Strategy
The siloed approach to strategy and planning for the issues that Aboriginal and Torres Strait Islander people face is a barrier to improvement. Whilst absolutely critical to closing the gap, the social determinants of health and wellbeing – from housing, education, employment and community support – are not adequately or comprehensively addressed.
The next Federal Government must prioritise the development of a National Aboriginal and Torres Strait Islander Social Determinants of Health Strategy that takes a broader, holistic look at the elements to health and wellbeing for Australia’s First Peoples. The Strategy must be developed in partnership with Aboriginal and Torres Strait Islander people through their peak organisations.
Please note the balance of document can be read here
Redfern Statement June 2016 Elections 18 Pages

#HealthElection16
Advertising and editorial is invited from
All political parties
NACCHO 150 Members and Affiliates
Stakeholders/ Aboriginal organisations
Peak Health bodies
Editorial Proposals Close 10 June 2016
Closing 17 June for publishing election week 29 June
Contact for Advertising rate cards/bookings/editorial

























{kind=link}